
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM
| REGISTRATION STATEMENT PURSUANT TO SECTION 12(b) OR (g) OF THE SECURITIES EXCHANGE ACT OF 1934 |
OR
| ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For
the fiscal year ended
OR
| TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
OR
| SHELL COMPANY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from _______________________ to ______________________________
Commission
File Number
(Exact name of Registrant as specified in its charter)
Scotland
(Jurisdiction of incorporation or organization)
Scotland,
+44 (0) 141 433 7557
(Address of principal executive offices)
Scotland,
(Name, Telephone, E-mail and/or Facsimile number and Address of Company Contact Person)
Securities registered or to be registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered | ||
Securities registered or to be registered pursuant to Section 12(g) of the Act: None
Securities for which there is a reporting obligation pursuant to Section 15(d) of the Act: None
Indicate the number of outstanding shares of each of the issuer’s classes of capital or common stock as of the close of the period covered by the annual report: ordinary shares, nominal value £0.01 per share.
Indicate
by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
If
this report is an annual or transition report, indicate by check mark if the registrant is not required to file reports pursuant to Section
13 or 15(d) of the Securities Exchange Act of 1934. Yes ☐
Indicate
by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange
Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2)
has been subject to such filing requirements for the past 90 days.
Indicate
by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule
405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant
was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or an emerging growth company. See definition of “large accelerated filer,” “accelerated filer” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer ☐ | Accelerated filer☐ | |||
| Emerging
growth company |
If
an emerging growth company that prepares its financial statements in accordance with U.S. GAAP, indicate by check mark if the registrant
has elected not to use the extended transition period for complying with any new or revised financial accounting standards† provided
pursuant to Section 13(a) of the Exchange Act.
† The term “new or revised financial accounting standard” refers to any update issued by the Financial Accounting Standards Board to its Accounting Standards Codification after April 5, 2012.
Indicate
by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness
of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered
public accounting firm that prepared or issued its audit report.
Indicate by check mark which basis of accounting the registrant has used to prepare the financial statements included in this filing:
| U.S. GAAP ☐ | by the International Accounting Standards Board ☒ |
Other ☐ |
If “Other” has been checked in response to the previous question, indicate by check mark which financial statement item the registrant has elected to follow. Item 17 ☐ Item 18 ☐
If
this is an annual report, indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange
Act). Yes ☐
TABLE OF CONTENTS
| 2 |
| 3 |
GENERAL INFORMATION
In this annual report on Form 20-F (“Annual Report”), unless the context requires otherwise, TC BioPharm (Holdings) plc (formerly TC BioPharm (Holdings) Limited, which was re-registered as a public limited company on January 10, 2022) and its subsidiaries (“Subsidiar(y/ies)”), and TC BioPharm Limited (our principal trading/operational subsidiary) shall collectively be referred to as “TCB,” “the Company,” “the Group”, “we,” “us,” and “our” unless otherwise noted.
PRESENTATION OF FINANCIAL AND OTHER DATA
The consolidated financial statement data as at December 31, 2021, 2020, and 2019 and for the years ended December 31, 2021, 2020 and 2019 have been derived from our consolidated financial statements, which have been prepared in accordance with International Financial Reporting Standards, or IFRS, as issued by the International Accounting Standards Board, or IASB and audited in accordance with the standards of the Public Company Accounting Oversight Board (United States).
Our financial information is presented in pounds sterling. For the convenience of the reader, in this Annual Report, unless otherwise indicated, translations from pounds sterling into U.S. dollars were made at the rate of £1.00 to $1.3500, which was the noon buying rate of the Federal Reserve Bank of New York on December 30, 2021. Such U.S. dollar amounts are not necessarily indicative of the amounts of U.S. dollars that could actually have been purchased upon exchange of pounds sterling at the dates indicated or any other date. All references in this Annual Report to “$” mean U.S. dollars and all references to “£” and “GBP” mean pounds sterling.
INFORMATION REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report contains estimates and forward-looking statements, principally in the sections titled “Risk Factors,” “Operating and Financial Review and Prospects” and “Business.” Some of the matters discussed concerning our operations and financial performance include forward-looking statements and estimates within the meaning of the Securities Act of 1933, as amended, and the Securities Exchange Act of 1934, as amended. The terminology such as “may,” “will,” “could,” “should,” “expects,” “anticipates,” “intends,” “plans,” “believes,” “seeks,” “estimates” and other comparable terminology are intended to identify forward-looking statements and estimates.
Forward-looking statements are subject to known and unknown risks, uncertainties, assumptions and other factors that could cause our actual results of operations, financial condition, liquidity, performance, prospects, opportunities, achievements or industry results, as well as those of the markets we serve or intend to serve, to differ materially from those expressed in, or suggested by, these forward-looking statements. Factors that could cause actual results, financial condition, liquidity, performance, prospects, opportunities, achievements or industry results to differ materially include, but are not limited to, those discussed under “Risk Factors” in this Annual Report. Additional risks that we may currently deem immaterial or that are not presently known to us could also cause the forward-looking events discussed in this Annual Report not to occur. These forward-looking statements are based on assumptions regarding our present and future business strategies and the environment in which we expect to operate in the future.
Forward-looking statements and estimates speak only at the date they were made, and we undertake no obligation to update or to review any forward-looking statement or estimate because of new information, future events or other factors. Forward-looking statements and estimates involve risks and uncertainties and are not guarantees of future performance. Our future results may differ materially from those expressed in these forward-looking statements and estimates.
WEBSITE DISCLOSURE
We maintain a public website at https://tcbiopharm.com and use our website as a routine channel of distribution of company information, including press releases, analyst presentations, and supplemental financial information, as a means of disclosing material non-public information and for complying with our disclosure obligations under Regulation FD. Our website includes an investors’ section through which we make available, free of charge, our Annual Reports on Form 20-F, Reports on Form 6-K, as well as any amendments to those reports filed or furnished pursuant to the Exchange Act as soon as reasonably practicable after we electronically file such material with, or furnish it to, the SEC. Accordingly, investors should monitor our website in addition to following press releases, filings with the SEC, and public conference calls and webcasts.
None of the information provided on our website, in our press releases or public conference calls and webcasts or through social media is incorporated into, or deemed to be a part of, this Annual Report or in any other report or document we file with the SEC, and any references to such website is intended to be inactive textual references only.
| 4 |
PART I
| Item 1. | Identity of Directors, Senior Management and Advisers |
Not Applicable.
| Item 2. | Offer Statistics and Expected Timetable |
Not Applicable.
| Item 3. | Key Information |
| A. | Selected Financial Data |
Not Applicable.
| B. | Capitalization and Indebtedness |
Not Applicable.
| C. | Reasons for the Offer and Use of Proceeds |
Not Applicable.
| 5 |
| D. | Risk Factors |
Investing in our company and its securities involves a high degree of risk. Investors should carefully consider the risks and uncertainties described below, together with all of the other information in this Annual Report, including our consolidated financial statements and related notes, before investing in our company and our securities. If any of the following risks materialize, our business, financial condition, operating results and prospects could be materially and adversely affected. In that event, the price or value of our ADSs and/or public Warrants in the public market could decline, and investors could lose part or all of their investment.
Summary of Risk Factors
Our business is subject to a number of risks and uncertainties, including those risks discussed at length in the section below titled “Risk Factors.” These risks include among others the following:
| ● | We have generated operating losses since inception and expect to continue to generate losses. We may never achieve or maintain profitability. We will continue to require financing to continue to implement our business plan and sustain operations. | |
| ● | We, as well as our independent registered public accounting firm, in relation to our financial position, have expressed substantial doubt about our ability to continue as a going concern. | |
| ● | Our lack of any approved products and our limited operating history may make it difficult for an investor to evaluate the success of our business to date and to assess our future viability. | |
| ● | GD-T cell therapies are a novel approach to treating cancers and viruses, which have development risks and will require us to obtain regulatory approvals for development, testing, commercialization, manufacturing and distribution. We may not achieve all the required regulatory approvals or approvals may not be obtained as timely as needed. | |
| ● | Because GD-T cell therapies are a novel approach, potential side effects, and long-term efficacy, regulatory approval will require considerable time for trials, data collection, regulatory submissions and funding for the process. | |
| ● | Enrolling patients in clinical trials may be difficult for many reasons, including high screen failure, GD-T cell proliferation capacity, timing, proximity and availability of clinical sites, perceived risks, and publicity about the success or lack of success in the methods of treatment. | |
| ● | Because GD-T cell therapies are novel, our research and development and clinical trial results may not support our products intended purposes and regulatory approval. We are heavily dependent on the success of our lead product candidate (OmnImmune®), and intend to seek breakthrough therapy designation for some or all of our other therapeutic candidates in due course. | |
| ● | Market opportunities for certain of our product candidates may be limited to those patients who are ineligible for or have failed prior treatments. This class of patient may be limited in number, difficult to locate and service, require special governmental approval, and unable to pay or obtain reimbursement. | |
| ● | We rely on many third parties for aspects of our product development and commercialization, such as raw material supply, clinical trials, obtaining approvals, aspects of manufacturing, development of additional product candidates and distribution. We may not be able to control these parties and their business practices, such as compliance with good manufacturing requirements or their ability to supply or service us timely, which will likely disrupt our business. | |
| ● | We face substantial competition: others may discover, develop and/or commercialize competing products before or more successfully than TCB. |
| 6 |
| ● | Even if we are able to commercialize any product candidates, such drugs may become subject to unfavorable pricing regulations or third-party coverage and reimbursement policies. Commercialized products may not be adopted by the medical profession. | |
| ● | Because we operate internationally, we are subject to a wide array of regulation of the United Kingdom, European Union and United States. In addition to regulation surrounding new drug development and their manufacture, distribution and use, we will be subject, for example to data protection rules relating to medical records, medical and general privacy laws, environmental laws regarding medical waste, and bribery and corrupt practices law, in addition to all the drug related approval, manufacturing and distribution rules. | |
| ● | Product liability claims are frequent in drug development of novel therapies and insurance is mandatory and expensive. The inability to obtain insurance may prevent product development and claims may surpass our ability to pay and call into question the efficacy of a product with resulting reputational damage. | |
| ● | Protecting our intellectual property is paramount in our ability to be able to commercialize our products and generate revenues and investment return for our stockholders. We may not be able to obtain the intellectual property protection we seek due to its cost, requirement to pursue it in many jurisdictions, challenges by others and patent office rejection. | |
| ● | Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies acting in multiple jurisdictions, and our patent protection could be reduced or eliminated for non-compliance with these requirements. | |
| ● | As part of product development, we may need to license aspects of our research and products from third parties or if our IP is challenged, we may have to seek license accommodation, any of which may be expensive, limited in scope, or unavailable. | |
| ● | We currently have a limited number of employees, and our future success depends on our ability to retain key executives and to attract, retain and motivate qualified personnel at all levels. | |
| ● | We will need to grow the size and capabilities of our organization, and we may experience difficulties in managing this growth including, but not limited to, operating as a public company and taking a therapeutic through to market approval and acceptance. | |
| ● | We expect to expand our development and regulatory capabilities and potentially implement sales, marketing and distribution capabilities, and as a result, we may encounter difficulties in achieving and managing our growth, which could disrupt our operations. We expect to require further funding for these expansions of activity. | |
| ● | We incur substantial costs as a result of operating as a public company in the United States, and our management is required to devote substantial time to required SEC compliance and corporate governance practices. | |
| ● | Certain of our existing stockholders, members of our board of directors and senior management maintain the ability to exercise significant control over us. The interests of investors may conflict with the interests of these other stockholders. | |
| ● | Our ADSs provide rights that are different from directly holding our ordinary shares. The outstanding public Warrants do not have the rights of shareholders until exercised. Our public Warrants form a substantial part of our capitalization, and they have substantial protective provisions, which may limit our ability to raise capital. | |
| ● | Future sales, or the possibility of future sales, of a substantial number of our ordinary shares, through the additional deposit of ordinary shares for ADSs and exercises of our public Warrants, could adversely affect the price of our ADSs or Warrants in the market. After any lock up period, a substantial number of our issued and outstanding ordinary shares will be eligible for trading on the public securities market by their being deposited with the depositary for ADSs. |
| 7 |
| ● | As a foreign private issuer, we, and our stockholders, have certain exceptions to disclosure regulation under United States federal securities regulation, and we will take certain NASDAQ governance exceptions. Consequently, investors may not have the totality of disclosure about and governance controls in TCB as compared to United States domestic reporting companies. | |
| ● | Shareholder rights and recourse will be governed by and ultimately determined by Scottish and United Kingdom law and judicial process, which in many ways are more limited than United States law and practice. Most of our directors and officers are not resident in the United States. Most of our assets are located in the United Kingdom. |
Risks Related to Our Financial Position and Need for Additional Capital
We have incurred net losses every year since our inception and expect to continue to incur net losses in the future and may never achieve profitability.
We have generated losses since our inception in 2013. Since then, we have devoted substantially all of our resources to research and development efforts relating to our genetically unmodified and genetically engineered GD-T cell candidates, including engaging in activities to manufacture and supply our GD-T cell candidates for clinical trials, conducting initial clinical trials of our lead candidates, general and administrative support for these operations, and protecting our intellectual property. Based on our current plans, we do not expect to generate product or royalty revenues until we obtain marketing approval for, and commercialize, any of our GD-T cell-based candidates.
For the fiscal years ended December 31, 2021 and 2020, we incurred net losses of £13.6 million ($18.3 million) and £5.5 million ($7.4 million), respectively. As of December 31, 2021, we had an accumulated deficit of £33.5 million ($45.2 million). We expect to continue incurring significant losses as we continue with our research and development and clinical programs and to incur general and administrative costs associated with our operations. The extent of funding required to develop our product candidates is difficult to estimate given the novel nature of our GD-T cell-based cell therapy candidates and their un-proven route to market. Ultimately, our profitability is dependent upon the successful development, approval, and commercialization of our GD-T cell-based therapeutic candidates and achieving a level of revenues adequate to support our cost structure. We may never achieve profitability and until we do, we will continue to need to raise additional cash.
Our ability to generate revenue from sales of our therapeutic candidates and become profitable depends significantly on our success in a number of factors.
We continue to focus on development activities for our technologies and implementation of the early parts of our business plan. A large percentage of our expenses will continue to be fixed; accordingly, our losses may be greater than expected and our operating results will suffer. We may never achieve commercial success and continue to operate in the research and development stage, without commercially launching any products at this time. We have limited historical financial data upon which we may base our projected revenue and base our planned operating expenses. Our limited operating history makes it difficult for potential investors to evaluate our potential product candidates, drug therapies or prospective operations and business prospects. As a development stage company, we are subject to all the risks inherent in the initial organization, business development, financing, unexpected expenditures, and complications and delays that often occur in a new business. Investors should evaluate an investment in us in light of the uncertainties encountered by developing companies in a competitive environment. There can be no assurance that our efforts will be successful or that we will ultimately be able to attain profitability.
We have no GD-T cell-based therapeutic candidates approved for commercial sale and have not generated any revenue from sales of our GD-T cell-based therapeutic candidates, and do not anticipate generating any revenue from sales of our GD-T cell-based therapeutic candidates until sometime after we receive regulatory approval, if at all, for the commercial sale of a GD-T cell-based therapeutic candidate. We intend to fund future operations through our existing and future collaboration and licensing agreements for other therapeutic targets and through additional equity financings. Our ability to generate revenue and achieve profitability depends on our success in many factors, including:
| ● | completing research regarding, and preclinical and clinical development of, our GD-T cell-based therapeutic candidates; |
| 8 |
| ● | obtaining regulatory approvals and marketing authorizations for our GD-T cell-based therapeutic candidates for which we complete clinical trials; | |
| ● | developing sustainable and scalable manufacturing and supply processes for our GD-T cell-based therapeutic candidates, including establishing and maintaining commercially viable supply relationships with third parties and pursuing our own commercial manufacturing capabilities and infrastructure; | |
| ● | launching and commercializing GD-T cell-based therapeutic candidates for which we obtain regulatory approvals and marketing authorizations, either directly or with a collaborator or distributor; | |
| ● | obtaining market acceptance of our GD-T cell-based therapeutic candidates as viable treatment options; | |
| ● | addressing any competing technological and market developments; | |
| ● | identifying, assessing, acquiring and/or developing new GD-T cell-based therapeutic candidates; | |
| ● | maintaining, protecting, and expanding our portfolio of intellectual property rights, including patents, trade secrets and know-how; and | |
| ● | attracting, hiring and retaining qualified personnel. |
Even if one or more of our GD-T cell-based therapeutic candidates is approved for commercial sale, we anticipate incurring significant costs associated with commercializing any approved GD-T cell-based therapeutic candidate. Our expenses will increase beyond our current expectations if the U.S. Food and Drug Administration, the FDA, or the United Kingdom Medicines and Healthcare products Regulatory Agency, the MHRA, or any other regulatory agency require changes to our manufacturing processes or assays, or for us to perform preclinical programs and clinical or other types of trials in addition to those that we currently anticipate. If we are successful in obtaining regulatory approvals to market one or more of our GD-T cell-based therapeutic candidates, our revenue will be dependent, in part, upon the size of the markets in the territories for which we gain regulatory approval, the accepted price for the GD-T cell-based therapeutic candidate, the ability to get reimbursement at any price, and whether we own the commercial rights for that territory. If the number of our addressable disease patients is not as significant as we estimate, the indication approved by regulatory authorities is narrower than we expect, or the reasonably accepted population for treatment is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenue from sales or supplies of such GD-T cell-based therapeutic candidates, even if approved. If we are not able to generate revenue from the sale of any approved GD-T cell-based therapeutic candidates, we may never become profitable.
If we fail to obtain additional financing as needed, we may be unable to complete the development and commercialization of our GD-T cell-based product candidates.
Our operations have required substantial amounts of cash since inception. We expect to continue to spend substantial amounts to continue the development of our GD-T cell-based therapeutic candidates, including for future clinical trials. We expect to use our operating capital to advance and accelerate the clinical development of our therapeutic candidates, therefore, changing circumstances beyond our control may cause us to increase our spending significantly faster than we currently anticipate, we believe we will require additional capital, likely in significant amounts, for the further development and commercialization of our GD-T cell-based therapeutic candidates.
| 9 |
We cannot be certain that additional funding will be available on acceptable terms, or at all. We have no committed source of additional capital. If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly delay, scale back or discontinue the development or commercialization of our GD-T cell-based therapeutic candidates or other research and development initiatives. Our license and supply agreements may also be terminated if we are unable to meet the milestone obligations under these agreements. We could be required to seek collaborators for our GD-T cell-based therapeutic candidates at an earlier stage than otherwise would be desirable or on terms that are less favorable than might otherwise be available or relinquish or license on unfavorable terms our rights to our GD-T cell-based therapeutic candidates in markets where we otherwise would seek to pursue development or commercialization ourselves. Any of the above events could significantly harm our business, prospects, financial condition and results of operations and cause the price of either of our ADSs or Warrants, or both, to decline.
We, as well as our independent registered public accounting firm, have expressed substantial doubt about our ability to continue as a going concern.
Our recurring losses from operations and negative cash flow raise substantial doubt about our ability to continue as a going concern. As a result, our independent registered public accounting firm included an explanatory paragraph in its report on our financial statements for the years ended December 31, 2020 and 2021 with respect to this uncertainty.
Our ability to continue as a going concern ultimately is dependent upon our generating cash flow from sales that are sufficient to fund operations or finding adequate financing to support our operations. To date, we have had no product revenues and relied on equity-based financing from the sale of securities subscribed by our founders and related parties and in various private placements, and receipts from collaboration partners. Our research and development plans may not be successful in creating a marketable product, and our business plan may not be successful in achieving a sustainable business and generating revenues. We completed our initial public offering (“IPO”) in February 2022, which, together with additional funds that we plan to raise during 2022, we believe will provide funding to enable us to progress our planned clinical trial program in our lead product, OmnImmune®, through the end of 2022. We have no firm arrangements in place for all the anticipated, required financing to be able to fund our operations during and beyond 2022 and otherwise to implement fully our business plan. If we are unable to continue as planned currently, we may have to curtail some or all of our business plan and operations. In such case, investors will lose all or a portion of their investment.
We anticipate needing additional financing over the longer term to execute our business plan and fund operations, which additional financing may not be available on reasonable terms or at all.
The proceeds from our February 2022 IPO, together with additional capital that we plan to raise during 2022, are expected to provide capital to further develop our drug product candidates and fund our overall business plan until at least the end of 2022. We will require additional capital in the future to fully develop our technologies and potential products to the stage of a commercial launch. We cannot give now any indication of the amount of future funding that we will need or give any assurance that we will be able to obtain all the necessary funding that we may need. We may pursue additional funding through various financing sources, including the private and public sale of our equity and debt securities, licensing fees for our product candidates, joint ventures with capital partners and project type financing. We also may seek government-based financing, such as development and research grants. There can be no assurance that funds will be available on commercially reasonable terms, if at all. If financing is not available on satisfactory terms, we may be unable to pursue further our business plan and we may be unable to continue operations, in which case investors may lose their entire investment. Alternatively, we may consider changes in our business plan that might enable us to achieve aspects of our business objectives and lead to some commercial success with a smaller amount of capital, but we cannot assure that changes in our business plan will result in revenues or maintain value in an investment in the company.
| 10 |
Risks Related to Development, Clinical Testing and Commercialization of Our Investigational Therapies and Any Future Therapeutic Candidates
Our GD-T cell therapies represent a novel approach to cancer and virus treatment that could result in heightened regulatory scrutiny, delays in clinical development, or delays in or our ability to achieve regulatory approval or commercialization of our therapeutic candidates.
Our products are novel cancer and virus treatment approaches that carry inherent development risks. We are therefore constantly evaluating and adapting our therapeutic candidates following the results obtained during development work and the ongoing clinical trials. Further development, characterization and evaluation may be required, depending on the results obtained, in particular where such results suggest any potential safety risk for patients. The need to develop further assays, or to modify in any way the protocols related to our therapeutic candidates to improve safety or effectiveness, may delay a clinical program, regulatory approval or commercialization, if approved at all, of any therapeutic candidate. Consequently, this may have a material impact on our ability to receive milestone payments and/or generate revenues from our therapeutic candidates. In addition, given the novelty of our GD-T cell therapeutic candidates, the end users and medical personnel require a substantial amount of education and training in their administration of our cell therapy. Regulatory authorities have very limited experience with commercial cell therapies for disease treatment. As a result, regulators may be more risk averse or require substantial dialogue and education as part of the normal regulatory approval process for each stage of development of our therapeutic candidates.
GD-T cell therapy creates significantly increased risk in terms of side-effect profile, ability to satisfy regulatory requirements associated with clinical trials, and the long-term efficacy of administered cells.
Development of a pharmaceutical or biologic therapy product has inherent risks based on differences in patient population and responses to therapy and treatment. The mechanism of action and impact on other systems and tissues within the human body following administration of GD-T cell therapy products is not completely understood, which means that we cannot predict the long-term effects of treatment with the GD-T cell therapy product. We are aware that certain patients may not respond to GD-T cell therapy and other patients may relapse. The percentage of the patient population in which these events may occur is unknown, but the inability of patients to respond and the possibility of relapse may impact our ability to conduct clinical trials, to obtain regulatory approvals, if at all, and to successfully commercialize our therapeutic products.
Our GD-T cell therapeutic candidates and their application are not fully scientifically understood and are still undergoing validation and investigation. The utility of our GD-T cell products may depend on persistence, potency, durability and infiltration capacity of the GD-T cells within a patient’s body. The level of persistence and the factors affecting such persistence, potency and infiltration capacity in patients are not completely understood, which presents an additional risk to the ongoing development and use of our therapeutic candidates. Certain steps involved in validating and carrying out testing require access to samples (for example tissue samples or cell samples) from third parties. Such samples may be obtained from universities or research institutions and will often be provided subject to satisfaction of certain terms and conditions. There can be no guarantee that we will be able to obtain samples in sufficient quantities to enable development of and use of the full preclinical safety testing program for CAR-T therapeutic candidates undergoing development. In addition, the terms under which such samples are available may not be acceptable to us or may restrict our use of any generated results or require us to make payments to the third parties.
Our products, before they can be commercialized, will require regulatory approval.
We cannot commercialize a product candidate until the appropriate regulatory authorities have reviewed and approved the product candidate. Approval by the FDA, the MHRA and comparable other regulatory authorities is lengthy and unpredictable, and depends upon numerous factors. Approval policies, regulations, or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions, which may cause delays in the approval or the decision not to approve an application. We have not obtained commercialization regulatory approval for any product candidate, and it is possible that any of our product candidates will never obtain regulatory approval.
Applications for product candidates we may develop could fail to receive regulatory approval for many reasons, including but not limited to:
| ● | our inability to demonstrate to the satisfaction of the regulatory authorities that a product candidate we develop is safe and effective; | |
| ● | the regulatory authorities may disagree with the design or implementation of our clinical trials; |
| 11 |
| ● | the population studied in the clinical program may not be sufficiently broad or representative to assure safety in the full population for which we seek approval; | |
| ● | the regulatory authorities’ requirement for additional preclinical studies or clinical trials; | |
| ● | the regulatory authorities may disagree with our interpretation of data from nonclinical studies or clinical trials; | |
| ● | the data collected from clinical trials may not be sufficient to support the submission of a new drug application, or NDA, or other submission for regulatory approval; | |
| ● | we may be unable to demonstrate to the regulatory authorities that a product candidate’s risk-benefit ratio for its proposed indication is acceptable; | |
| ● | the regulatory authorities may fail to approve the manufacturing processes, test procedures and specifications, or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; and | |
| ● | the approval policies or regulations of the regulatory authorities may change in a manner that renders our clinical trial design or data insufficient for approval. |
The lengthy approval process, as well as the unpredictability of the results of clinical trials, may result in our failing to obtain regulatory approval to market a product candidate in the United States, the UK, the EU or elsewhere, which would significantly harm our business, prospects, financial condition and results of operations.
We may encounter substantial delays in completing our clinical trials, which in turn will result in additional costs and may ultimately prevent successful or timely completion of the clinical development and commercialization of our product candidates.
We must conduct extensive clinical trials to demonstrate the safety and efficacy of the product candidates in humans before commercialization. Clinical testing is expensive, time-consuming and uncertain as to outcome. We cannot guarantee that any clinical trials will be conducted as planned or completed on schedule, if at all. A failure of one or more clinical trials can occur at any stage of testing. Events that may prevent successful or timely completion of clinical development include:
| ● | delays in reaching, or any failure to reach, a consensus with regulatory agencies on study design; | |
| ● | delays in obtaining FDA required Institutional Review Board, or IRB, approval at each clinical trial site; | |
| ● | delays in recruiting a sufficient number of suitable patients to participate in our clinical trials; | |
| ● | imposition of a clinical hold by regulatory agencies, after an inspection of our clinical trial operations or study sites; |
| ● | failure by third parties or us to adhere to clinical trial, regulatory or legal requirements; | |
| ● | failure to perform in accordance with good clinical practices, GCP, or applicable regulatory guidelines in other countries; | |
| ● | delays in the testing, validation, manufacturing and delivery of sufficient quantities of our product candidates to the clinical sites; | |
| ● | delays in having patients’ complete participation in a study or return for post-treatment follow-up; |
| 12 |
| ● | clinical trial sites or patients dropping out of a trial; | |
| ● | delay or failure to address any patient safety concerns that arise during the course of a trial; | |
| ● | unanticipated costs or increases in costs of clinical trials of our product candidates; | |
| ● | occurrence of serious adverse events associated with the product candidate that are viewed to outweigh its potential benefits; or | |
| ● | changes in regulatory requirements and guidance that require amending or submitting new clinical protocols. |
We could also encounter delays if a clinical trial is suspended or terminated by us or by regulators and related reviewing authorities such as IRBs of the institutions in which such trials are being conducted, by an independent Safety Review Board. Suspension or termination of a clinical trial might be due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, or failure to demonstrate a benefit from using a therapy. In addition, if we make manufacturing or formulation changes to our product candidates, we may need to conduct additional studies to bridge our modified product candidates to earlier versions. In addition, any delays in completing our clinical trials will increase our costs, slow down our product candidate development and approval process and jeopardize our ability to obtain regulatory approvals, commence product sales and generate revenues. Any of these occurrences may significantly harm our business, prospects, financial condition and results of operations.
Manufacturing and administering our GD-T cell-based therapeutic candidates is complex, and we may encounter difficulties in production, particularly with respect to process development or scaling-up of our manufacturing capabilities. If we encounter such difficulties, our ability to supply of our GD-T cell therapeutic candidates for clinical trials or for commercial purposes could be delayed or stopped.
Manufacturing and administrating our GD-T cell-based therapeutics candidates is complex and highly regulated. The manufacture process of our GD-T cell-based therapeutics involves complex processes, including peripheral blood mononuclear cell isolation from leukapheresis material, stimulation of the GD-T cells, expansion of the cells to obtain a desired dose, and ultimately infusion of the cells to the patient’s body. On occasions the GD-T cell therapeutic could be genetically modified, which could involve manufacturing of lentiviral vectors containing the gene of our interest (for example Chimeric Antigen Receptor) and transducing the cells or a method such as electroporation or nucleofection of a plasmid containing the gene of interest to the cells. As a result of the complexities, our manufacturing and supply costs are likely to be higher than those in more traditional manufacturing processes and the manufacturing process is less reliable and more difficult to reproduce. Our manufacturing process is, and will be, susceptible to product loss or failure due to logistical issues, including manufacturing issues associated with the differences in patients’ white blood cells, interruptions in the manufacturing process, contamination, equipment or reagent failure, supplier error and variability in GD-T cell-based therapeutic candidate and patient characteristics. Even minor deviations from normal manufacturing processes could result in reduced production yields, product defects, and other supply disruptions. If microbial, viral or other contaminations are discovered in our GD-T cell-based therapeutic candidates or in the manufacturing facilities in which our GD-T cell based therapeutic candidates are made or administered, the manufacturing facilities may need to be closed for an extended period of time to investigate and remedy the contamination. As our GD-T cell-based therapeutic candidates progress through preclinical programs and clinical trials towards approval and commercialization, it is expected that various aspects of the manufacturing and administration process will be altered in an effort to optimize processes and results.
We have identified some improvements to our manufacturing and administration processes, but these changes may not achieve the intended objectives, and could cause our GD-T cell-based therapeutic candidates to perform differently and affect the results of planned clinical trials or other future clinical trials. The changes may require amendments to be made to regulatory applications which may further delay the timeframes under which modified manufacturing processes can be used for any GD-T cell-based therapeutic candidate. For example, we are planning to introduce automated enclosed systems to our production process. This will require development work to ensure that these modifications do not alter the characteristics of the product. If the GD-T cell-based therapeutic candidate manufactured under the new process has a worse safety or efficacy profile than the prior investigational product, we may need to re-evaluate the use of that manufacturing process, which could significantly delay the progress of our clinical trials.
| 13 |
Developing a commercially viable process is a difficult and uncertain task and there are risks associated with scaling to the level required for advanced clinical trials or commercialization, including, among others, increased costs, potential problems with process scale-out, process reproducibility, stability issues, lot consistency, and timely availability of reagents or raw materials. We may ultimately be unable to reduce the expenses associated with our GD-T cell-based therapeutic candidates to levels that will allow us to achieve a profitable return on investment. If we are unable to demonstrate that our commercial scale product is comparable to the product used in clinical trials, we may not receive regulatory approval for that product without additional clinical trials. Even if we are successful, our manufacturing capabilities could be affected by increased costs, unexpected delays, equipment failures, labor shortages, natural disasters, power failures and numerous other factors that could prevent us from realizing the intended benefits of our manufacturing strategy, which in turn could have a material adverse effect on our business.
We may seek expedited approval in the European Union and United States for our therapeutic candidates, but we may not be able to obtain or maintain such designation.
The FDA and the European Medicines Agency, the EMA, have established programs to expedite drug development and regulatory review. The FDA has four main expedited programs: fast track (introduced in 1987), accelerated approval (1992), priority review (1992), and breakthrough therapy (2012). A priority review designation in North America will direct overall attention and resources to the evaluation of applications for drugs that, if approved, would be significant improvements in the safety or effectiveness of the treatment, diagnosis, or prevention of serious conditions when compared to standard applications. Significant improvement may be demonstrated by the following examples:
| ● | evidence of increased effectiveness in treatment, prevention, or diagnosis of condition; | |
| ● | elimination or substantial reduction of a treatment-limiting drug reaction; | |
| ● | documented enhancement of patient compliance that is expected to lead to an improvement in serious outcomes; or | |
| ● | evidence of safety and effectiveness in a new subpopulation. |
We intend to seek breakthrough therapy designation for some or all of our therapeutic candidates, but there can be no assurance that we will receive breakthrough therapy designation. Additionally, other treatments from competing companies may obtain the designations and impact our ability to develop and commercialize our therapeutic candidates, which may adversely impact our business, financial condition or results of operation. We may also seek fast track designation. If a drug or biologic candidate is intended for the treatment of a serious or life-threatening condition or disease and the drug demonstrates the potential to address unmet medical needs for the condition, the sponsor may apply for fast track designation. Under the fast track program, the sponsor of a new drug or biologic candidate may request that the FDA designate the candidate for a specific indication as a fast track drug or biologic concurrent with, or after, the submission of the IND for the candidate. The FDA must determine if the drug or biologic candidate qualifies for fast track designation within 60 days of receipt of the sponsor’s request. Even if we do apply for and receive fast track designation, we may not experience a faster development, review or approval process compared to conventional FDA procedures. The FDA may withdraw fast track designation if it believes that the designation is no longer supported by data from our clinical development program. We may also seek accelerated approval for products that have obtained fast track designation. Under the FDA’s fast track and accelerated approval programs, the FDA may approve a drug or biologic for a serious or life-threatening illness that provides meaningful therapeutic benefit to patients over existing treatments based upon a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. For drugs granted accelerated approval, post-marketing confirmatory trials have been required to describe the anticipated effect on irreversible morbidity or mortality or other clinical benefit. These confirmatory trials must be completed with due diligence.
| 14 |
The EMA has three programs, the accelerated assessment (2005), conditional marketing authorization (2006), and the Priority Medicines (PRIME) scheme (2016). These programs are intended to prioritize the most important medicines for faster access by patients. As part of its marketing authorization process, the EMA may grant conditional marketing authorizations for certain categories of medicinal products on the basis of less complete data than is normally required, when doing so may meet unmet medical needs of patients and may serve the interest of public health. In these cases, it is possible for the Committee for Medicinal Products for Human Use, the CHMP, to recommend the granting of a marketing authorization, subject to certain specific obligations to be reviewed annually, which is referred to as a conditional marketing authorization. This may apply to medicinal products for human use that fall under the jurisdiction of the EMA, including those that aim at the treatment, the prevention, or the medical diagnosis of seriously debilitating diseases or life-threatening diseases and those designated as orphan medicinal products. A conditional marketing authorization may be granted when the CHMP finds that, although comprehensive clinical data referring to the safety and efficacy of the medicinal product have not been supplied, the risk-benefit balance of the medicinal product is positive. The granting of a conditional marketing authorization is restricted to situations in which only the clinical part of the application is not yet fully complete. Incomplete preclinical or quality data may only be accepted if duly justified and only in the case of a product intended to be used in emergency situations in response to public-health threats. Conditional marketing authorizations are valid for one year, on a renewable basis. The holder will be required to complete ongoing trials or to conduct new trials with a view to confirming that the benefit-risk balance is positive. In addition, specific obligations may be imposed in relation to the collection of pharmacovigilance data. Granting a conditional marketing authorization allows medicines to reach patients with unmet medical needs earlier than might otherwise be the case and will ensure that additional data on a product are generated, submitted, assessed and acted upon. Although we may seek a conditional marketing authorization for our therapeutic candidates, the EMA or CHMP may ultimately not agree that the requirements for conditional marketing authorization have been satisfied and hence delay the commercialization of our therapeutic candidates.
In the European Union, accelerated assessment can reduce the timeframe for EMA’s CHMP to review a marketing-authorization application. Applications may be eligible for accelerated assessment if the CHMP decides the product is of major interest for public health and therapeutic innovation. The evaluation of a marketing-authorization application can take up to 210 days. However, the CHMP can reduce the timeframe to 150 days if the applicant can provide sufficient justification for an accelerated assessment. The Priority Medicines (PRIME) scheme was introduced by the EMA in 2016 to support the development of medicines addressing unmet medical needs which offer a therapeutic advantage over existing treatments. To be accepted in the PRIME scheme, the treatments must meet the eligibility criteria for accelerated assessment including a strongly substantiated mechanism of action, supportive preclinical data, and first-in-human tolerance data. PRIME has been compared to the U.S. Breakthrough Therapy Designation.
Withdrawal of expedited approval will delay trials and likely increase cost.
The FDA or EMA may withdraw expedited approval of our therapeutic candidate or indication approved under the accelerated approval pathway if, for example:
| ● | the trial or trials required to verify the predicted clinical benefit of our therapeutic candidate fail to verify such benefit or do not demonstrate sufficient clinical benefit to justify the risks associated with the drug; | |
| ● | other evidence demonstrates that our therapeutic candidate is not shown to be safe or effective under the conditions of use; | |
| ● | we fail to conduct any required post-approval trial of our therapeutic candidate with due diligence; or | |
| ● | we disseminate false or misleading promotional materials relating to the relevant therapeutic candidate. |
| 15 |
Obtaining and maintaining regulatory approval of our therapeutic candidates in one jurisdiction does not mean that we will be successful in obtaining regulatory approval of our therapeutic candidates in other jurisdictions.
We plan on submit marketing applications in multiple jurisdictions and countries, including the UK, the EU and the United States. Regulatory authorities in each jurisdiction have requirements for approval of therapeutic candidates with which we must comply prior to marketing in those jurisdictions. Obtaining regulatory approvals and compliance with regulatory requirements of multiple jurisdictions and countries could result in significant delays, difficulties and costs for us and could delay or prevent the introduction of our therapeutic candidates in certain countries. If we fail to comply with the regulatory requirements in international markets and/or receive applicable marketing approvals, our target market will be reduced and our ability to realize the full market potential of our therapeutic candidates will be harmed.
Obtaining and maintaining regulatory approval of our therapeutic candidates in one jurisdiction does not guarantee that we will be able to obtain or maintain regulatory approval in any other jurisdiction, while a failure or delay in obtaining regulatory approval in one jurisdiction may have a negative effect on the regulatory approval process in others. For example, even if the FDA grants marketing approval of our key products in the United States, comparable regulatory authorities in other jurisdictions must also approve the manufacturing, marketing and promotion of our products in those countries. Approval procedures vary among jurisdictions and may require additional preclinical programs or clinical trials. In many jurisdictions a therapeutic candidate must be approved for reimbursement before it can be approved for sale in that jurisdiction. In some cases, the price that we intend to charge for our therapeutic candidates is also subject to approval.
We may face difficulty in enrolling patients in our clinical trials.
We may find it difficult to enroll patients in our clinical trials. For example, in our TCB-001 clinical trial we experienced a high screen failure rate. Identifying and qualifying patients, including testing of patients for their GD-T cells’ proliferation capacity, to participate in clinical trials of our therapeutic candidates, are critical to our success. The timing of our current and future clinical trials depends on the speed at which we can recruit patients to participate in testing our therapeutic candidates. If patients are unwilling to participate in our trial(s) because of negative publicity from adverse reactions or for other reasons, including competitive clinical trials for similar patient populations, the timeline for recruiting patients, conducting trials and obtaining regulatory approval of potential products may be delayed or prevented. These delays could result in increased costs, delays in advancing our product development, delays in testing the effectiveness of our technology or termination of the clinical trials altogether. We may not be able to identify, recruit and enroll a sufficient number of patients, or those with required or desired characteristics to achieve sufficient diversity in a given trial in order to complete our clinical trials in a timely manner. Patient enrolment is affected by factors including:
| ● | eligibility criteria for the trial in question; | |
| ● | severity of the disease under investigation; | |
| ● | design of the trial protocol; | |
| ● | trial duration and number and complexity of visits and procedures; | |
| ● | size of the patient population; | |
| ● | perceived risks and benefits of the therapeutic candidate under trial; | |
| ● | novelty of the therapeutic candidate and acceptance by oncologists; | |
| ● | proximity and availability of clinical trial sites for prospective patients; | |
| ● | availability of competing therapies and clinical trials; | |
| ● | efforts to facilitate timely enrolment in clinical trials; |
| 16 |
| ● | patient referral practices of physicians; and | |
| ● | ability to monitor patients adequately during and after treatment. |
If we have difficulty enrolling a sufficient number of patients to conduct our clinical trials as planned, we may need to delay, limit or terminate ongoing or planned clinical trials, any of which would have an adverse effect on our business.
The outcome of clinical trials is uncertain and our clinical trials may fail to demonstrate adequately the safety and efficacy of any of our T cell therapeutic candidates, which would prevent or delay regulatory approval and commercialization.
There is a risk in any clinical trial that side effects from our therapeutic candidates will require a hold on, or termination of, our clinical program(s) or further adjustments to our clinical program(s) in order to progress our therapeutic candidates. Our T cell therapeutic candidates will require evidence that they are safe before permitting clinical trials to commence and evidence that the therapeutic candidates are safe and effective before granting any regulatory approval. In particular, because our therapeutic candidates are subject to regulation as biological products, we will need to demonstrate that they are safe, pure and potent for use in each target indication. The therapeutic candidate must demonstrate an acceptable risk versus benefit profile in its intended patient population and for its intended use. The risk/benefit profile required for product licensure will vary depending on these factors and may include not only the ability to show tumor shrinkage, but also adequate duration of response, a delay in the progression of the disease and/or an improvement in survival. For example, response rates from the use of our therapeutic candidates will not be sufficient to obtain regulatory approval unless we can also show an adequate duration of response.
We may not be able to submit INDs, or the foreign equivalent outside of the United States, to continue our CAR-T clinical trials.
We are currently conducting preclinical development of our CAR-T therapeutic candidates. Progression of our CAR-T therapeutic candidates from pre- to clinical development (first-in-human, phase 1) is inherently risky and dependent on the results obtained in preclinical programs, the results of other clinical programs and results of third-party programs that utilize common components used for production and administration of our therapeutic candidates. If results are not available when expected or problems are identified during therapy development, we may experience significant delays in development of pipeline products and of existing clinical programs, which may impact our ability to receive regulatory approval. This may also impact our ability to achieve certain financial milestones and the expected timeframes to market any of our therapeutic candidates. Failure to submit further INDs or the foreign equivalent and commence additional clinical programs will significantly limit our opportunity to generate revenue.
Our research and development efforts may not result in the progression of our product candidates into clinical trials.
Our research and development efforts and our selection of the product candidates to pursue remain subject to all of the risks associated with the development of new treatment modalities. Development of the underlying technology may be affected by unanticipated technical or other problems, among other development and research issues, and the possible insufficiency of funds needed in order to complete development of these products. Safety, regulatory and efficacy issues, clinical hurdles or challenges also may result in delays and cause us to incur additional expenses that will increase our need for capital and result in additional losses. If we cannot complete, or if we experience significant delays in developing our medical products for use in potential commercial applications, particularly after incurring significant expenditures, our business may fail and investors may lose the entirety of their investment.
| 17 |
We will need to obtain regulatory approval for our product candidates, which is time consuming, costly and complicated. We may not obtain regulatory approval.
We cannot commercialize a product candidate until the appropriate regulatory authorities have reviewed and approved the product candidate. Approval by the FDA and comparable foreign regulatory authorities is lengthy and unpredictable, and depends upon numerous factors. Approval policies, regulations, or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions, which may cause delays in the approval or the decision not to approve an application. We have not obtained regulatory approval for any product candidate, and it is possible that any of our product candidates will never obtain regulatory approval.
Applications for product candidates we may develop could fail to receive regulatory approval for many reasons. For example, under FDA regulation, approval may not be obtained for many reasons such as:
| ● | our inability to demonstrate to the satisfaction of the FDA or comparable foreign regulatory authorities that a product candidate we may develop is safe and effective; | |
| ● | the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our clinical trials; | |
| ● | the population studied in the clinical program may not be sufficiently broad or representative to assure safety in the full population for which we seek approval; | |
| ● | the FDA’s or comparable foreign regulatory authorities’ requirement for additional preclinical studies or clinical trials; | |
| ● | the FDA or comparable foreign regulatory authorities may disagree with our interpretation of data from nonclinical studies or clinical trials; |
| ● | the data collected from clinical trials of our product candidates may not be sufficient to support the submission of a new drug application, or NDA, or other submission for regulatory approval in the United States or elsewhere; | |
| ● | we may be unable to demonstrate to the FDA or comparable foreign regulatory authorities that a product candidate’s risk-benefit ratio for its proposed indication is acceptable; | |
| ● | the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes, test procedures and specifications, or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; and | |
| ● | the approval policies or regulations of the FDA or comparable foreign regulatory authorities may change in a manner that renders our clinical trial design or data insufficient for approval. |
The lengthy approval process, as well as the unpredictability of the results of clinical trials, may result in our failing to obtain regulatory approval to market a product candidate in the United States or elsewhere, which would significantly harm our business, prospects, financial condition and results of operations
We are heavily dependent on the success of our lead product candidate, OmnImmune®, and our subsequent product development program, If we are unable to successfully complete clinical development, obtain regulatory approval for, or commercialize these products, or experience delays in doing so, our business will be materially harmed.
Our future success is dependent on our ability to successfully develop, obtain regulatory approval for, and commercialize our aforementioned lead product candidate which is in its clinical development phase. Before we can generate any revenues from sales of products, we will be required to conduct additional clinical development and conduct longer-term clinical trials and, if our clinical trial of these products is successful, we will be required to seek and obtain regulatory approval, secure adequate manufacturing supply to support larger clinical trials and commercial sales and build a commercial organization, or to work with commercilaisation partners. Further, the success of these products will depend on patent and trade secret protection, acceptance of these products by patients, the medical community and third-party payers, its ability to compete with other therapies, healthcare coverage and reimbursement, and maintenance of an acceptable safety profile following approval, among other factors. If we do not achieve any of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully commercialize our products which would materially harm our business.
| 18 |
Laboratory conditions differ from clinical conditions and commercial conditions, which could affect the effectiveness of our potential products. Failures to effectively move from laboratory to the field would harm our business.
Observations and developments that may be achievable under laboratory circumstances may not be replicated in commercial settings or in the use of any of the proposed products in the field. The failure of our product candidates under development or other future product candidates to be able to be tested, approved and manufactured in available manufacturing facilities or to be able to meet the demands of users in the field would harm our business.
Results of earlier studies may not be predictive of future clinical trial results, and initial studies may not establish an adequate safety or efficacy profile for our drugs and other product candidates that we may pursue to justify proceeding to advanced clinical trials or an application for regulatory approval.
The results of preclinical studies and clinical trials of our product candidates may not be predictive of the results of later-stage clinical trials, and interim results of a clinical trial do not necessarily predict final results. Additionally, any positive results generated in our Phase 1b/2a clinical trials in adults would not ensure that we will achieve similar results in larger, pivotal clinical trials or in clinical trials in general populations. In addition, preclinical and clinical data are often susceptible to various interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy despite having progressed through nonclinical studies and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier studies, and we cannot be certain that we will not face similar setbacks. Even if early-stage clinical trials are successful, we may need to conduct additional clinical trials for product candidates in additional patient populations or under different treatment conditions before we are able to seek approvals from the FDA and regulatory authorities outside the United States to market and sell these product candidates. Our failure to demonstrate the required characteristics to support marketing approval for our product candidates in any ongoing or future clinical trials would substantially harm our business, prospects, financial condition and results of operations.
We manufacture and test all our therapeutic candidates in-house, and may experience logistic issues.
The manufacture, testing and release of TCB’s cell therapies for clinical trials may not meet with the regulatory requirements and result in the delay of clinical trials. Logistical issues which may prevent timely completion of manufacture and testing include:
| ● | failure in integrity of facility infrastructure; | |
| ● | failure of High Efficiency Particulate Absorbing (HEPA) filters to prevent airborne cross-contamination; | |
| ● | delays in the procuring test materials/reagents due to supplier, shipping issues or discontinued supply; | |
| ● | failure by third parties to notify a change in material product specifications that are not GMP compliant; | |
| ● | redundant equipment (or parts) used within the manufacturing process; | |
| ● | equipment failure within production, quality control and stores; | |
| ● | failure of quality control equipment; |
| 19 |
| ● | delays in cleanroom supplies from third parties such as PPE or cleaning reagents; | |
| ● | failure in the cleanroom resulting in insufficient quantities of our product candidates being available to the clinical sites; | |
| ● | increase in our costs of materials; | |
| ● | delays in final product release testing being conducted within product shelf-life of 36 hours; | |
| ● | released in ‘real time’ which means that safety testing is incomplete when administered to the patient resulting in contaminated product being released to the clinic; | |
| ● | failure due to resource issues associated with personnel illness; and | |
| ● | failure in recruitment of cleanroom operators and quality staff as we progress through clinical trials. |
We conduct and manage clinical studies using internal staff trained to perform such studies and loss of these staff may delay our clinical program.
We are highly dependent upon the principal members of our management team and the members of our scientific team. These persons have significant experience and knowledge within our operational sector, and the loss of any team member could impair our ability to design, identify, and develop clinical trials, new intellectual property and new scientific or product ideas.
We expect to operate in a highly competitive, ever evolving, market.
The broader market for our products is becoming more focused and potentially more competitive. Over time, we believe this field will become subject to more rapid change and new drugs, therapies and other products will emerge. We may not be able to compete effectively against these companies or their products. We may find ourselves in competition with companies that have competitive advantages over us, such as:
| ● | significantly greater name recognition; | |
| ● | established relations with healthcare professionals, customers and third-party payors; | |
| ● | established distribution networks; | |
| ● | additional lines of products, and the ability to offer rebates, higher discounts or incentives to gain a competitive advantage; | |
| ● | greater experience in conducting research and development, manufacturing, clinical trials, obtaining regulatory approval for products, and marketing approved products; and | |
| ● | greater financial and human resources for product development, sales and marketing, and patent litigation. |
Many of our competitors, either alone or with their strategic collaborators, have substantially greater financial, technical and human resources than we do. Accordingly, our competitors may be more successful than we are in obtaining approval for treatments and achieving widespread market acceptance and may render our treatments obsolete or non-competitive. Mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated among a smaller number of our competitors. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical study sites and patient registration for clinical studies, as well as in acquiring technologies complementary to, or necessary for, our programs. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
| 20 |
Rapidly changing medical technology within the life sciences could make the product candidates that we are developing obsolete.
The medical industry is characterized by rapid and significant medical technological and therapy changes, frequent new product candidates and product introductions and enhancements and evolving industry standards. Our future success will depend on our ability to continually develop and then improve the product candidates that we design and to develop and introduce new product candidates that address the evolving needs of the physicians and patients on a timely and cost-effective basis. Any new product candidates and products developed by us may not be accepted in the intended markets. Our inability to gain market acceptance of new products could harm our future operating results.
The market opportunities for certain of our product candidates may be small, due to the fact that the products may be limited to those patients who are ineligible for or have failed prior treatments, and our projections regarding the size of the addressable market may be incorrect.
Cancer therapies are sometimes characterized as first line, second line or third line, and the FDA often approves new therapies initially only for third line use. When blood cancers are detected, they are treated with first line of therapy with the intention of curing the cancer. This generally consists of chemotherapy, radiation, antibody drugs, tumor targeted small molecules, or a combination of these. In addition, sometimes a bone marrow transplantation can be added to the first line therapy after the combination chemotherapy is given. If the patient’s cancer relapses, then they are given a second line or third line therapy, which can consist of more chemotherapy, radiation, antibody drugs, tumor targeted small molecules, or a combination of these, or bone marrow transplant. Generally, the higher the line of therapy, the lower the chance of a cure. With third or higher line, the goal of the therapy in the treatment of lymphoma and myeloma is to control the growth of the tumor and extend the life of the patient, as a cure is unlikely to happen. Patients are generally referred to clinical trials in these situations.
Our projections of both the number of people who have the cancers we are targeting, as well as the size of the patient population subset of people with these cancers in a position to receive first, second, third and fourth line therapy and who have the potential to benefit from treatment with our product candidates, are based on our beliefs and estimates. These estimates have been derived from a variety of sources, including scientific literature, surveys of clinics, patient foundations, or market research and may prove to be incorrect. Further, new studies may change the estimated incidence or prevalence of these cancers. The number of patients may turn out to be fewer than expected. Additionally, the potentially addressable patient population for our product candidates may be limited or may not be amenable to treatment with our product candidates. Even if we obtain significant market share for our product candidates, because the potential target populations are small, we may never achieve significant revenues without obtaining regulatory approval for additional indications or as part of earlier lines of therapy.
We rely on third parties to support our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval of or commercialize our product candidates.
We depend and will continue to depend upon independent investigators and collaborators, such as universities, medical institutions, CROs and strategic partners to support our clinical trials under agreements with the Company.
We negotiate budgets and contracts with CROs and study sites, which may result in delays to our development timelines and increased costs. We will rely heavily on third parties over the course of our clinical trials, and we control only certain aspects of their activities. Nevertheless, we are responsible for ensuring that each of our studies is conducted in accordance with applicable protocol, legal, regulatory and scientific standards, and its reliance on third parties does not relieve us of our regulatory responsibilities. TCB and these third parties are required to comply with GCPs, which are regulations and guidelines enforced by regulatory authorities for product candidates in clinical development. Regulatory authorities enforce these GCPs through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of these third parties fail to comply with applicable GCP regulations, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure that, upon inspection, such regulatory authorities will determine that any of our clinical trials comply with the GCP regulations. In addition, our clinical trials must be conducted with biologic product produced under cGMPs and will require a large number of test patients. Our failure or any failure by these third parties to comply with these regulations or to recruit a sufficient number of patients may require us to repeat clinical trials, which would delay the regulatory approval process. Moreover, our business may be implicated if any of these third parties violates federal or state fraud and abuse or false claims laws and regulations or healthcare privacy and security laws.
| 21 |
Any third parties supporting our clinical trials are and will not be our employees and, except for remedies available to us under our agreements with such third parties, we cannot control whether or not they devote sufficient time and resources to our ongoing preclinical, clinical and nonclinical programs. These third parties may also have relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical studies or other drug development activities, which could affect their performance on our behalf. If these third parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to complete development of, obtain regulatory approval of or successfully commercialize our product candidates. As a result, our financial results and the commercial prospects for our product candidates would be harmed, our costs could increase and our ability to generate revenue could be delayed.
If any of our relationships with trial sites, or any CRO that we may use in the future, terminates, we may not be able to enter into arrangements with alternative trial sites or CROs or do so on commercially reasonable terms. Switching or adding third parties to conduct our clinical trials will involve substantial cost and require extensive management time and focus. In addition, there is a natural transition period when a new third party commences work. As a result, delays occur, which can materially impact our ability to meet its desired clinical development timelines.
We do not have any current sales, marketing, commercial manufacturing and distribution capabilities or arrangements, and will need to create these as we move towards commercialization of our products.
We do not yet have commercial sales, marketing, manufacturing and distribution capabilities or arrangements. We will need to develop all of the foregoing or partner with organizations who have expertise in all the foregoing. We do not have any corporate experience in establishing these commercial sized capabilities. We believe that setting up the commercialization aspects of a company such as ours, in our field, will take a substantial amount of capital and time. Therefore, we may seek development and marketing partners and license our drug technologies or product candidates to others in order to avoid our having to provide the marketing, manufacturing and distribution capabilities within our organization. There can be no assurance that we will find any development and marketing partners or companies that are interested in licensing our drug technology or any of our product candidates or products. If we are unable to establish and maintain adequate sales, marketing, manufacturing and distribution capabilities, independently or with others, we will not be able to generate product revenue, and may not become profitable.
We may rely on third parties to manufacture our clinical product supplies, and we may have to rely on third parties to produce and process our product candidates, if approved.
Although to date, we have used our internal capabilities to manufacture clinical trial supplies, we do not yet have sufficient information to reliably estimate the cost of commercially manufacturing and processing of our product candidates. The actual cost to manufacture and process our product candidates could materially and adversely affect the commercial viability of our product candidates. As a result, we may never be able to develop a commercially viable product.
We anticipate that we will rely on a limited number of third-party manufacturers for commercial production, but this will expose us to the following risks.
| ● | We may be unable to identify manufacturers on acceptable terms or at all because the number of potential manufacturers is limited and the regulatory authorities may have questions regarding any replacement contractor. This may require new testing and regulatory interactions. In addition, a new manufacturer would have to be educated in, or develop substantially equivalent processes for, production of our products. |
| 22 |
| ● | Third-party manufacturers might be unable to timely formulate and manufacture our product or produce the quantity and quality required to meet our clinical and commercial needs, if any. | |
| ● | Future contract manufacturers may not perform as agreed or may not remain in the contract manufacturing business for the time required to supply our clinical trials or to successfully produce, store and distribute our products. | |
| ● | Manufacturers are subject to strict compliance with cGMP and other government regulations and corresponding foreign standards. We do not have control over third-party manufacturers’ compliance with these regulations and standards. | |
| ● | We may not own, or may have to share, the intellectual property rights to any improvements made by our third-party manufacturers in the manufacturing process for our products. | |
| ● | Third-party manufacturers could breach or terminate their agreement(s) with us. |
Contract manufacturers would also be subject to the same risks we face in developing our own manufacturing capabilities, as described above. Each of these risks could delay our clinical trials, the regulatory approval, if any, of our product candidates or the commercialization of our product candidates or result in higher costs or deprive us of potential product revenue. In addition, we will rely on third parties to perform release tests on our product candidates prior to delivery to patients. If these tests are not appropriately done and test data are not reliable, patients could be put at risk of serious harm.
Cell-based therapies rely on the availability of specialty raw materials, which may not be available to us on acceptable terms or at all.
Our product candidates require specialized raw materials, including viral vectors that deliver the targeting moiety (CAR) and other genes to the product candidate. We currently manufacture some of our requirements through contract manufacturers, some of which are manufactured by companies with limited resources and experience to support a commercial product, and the suppliers may not be able to deliver raw materials to our specifications. In addition, those suppliers normally support blood-based hospital businesses and generally do not have the capacity to support commercial products manufactured under cGMP by biopharmaceutical firms. The suppliers may be ill-equipped to support our needs, especially in non-routine circumstances like an FDA inspection or medical crisis, such as widespread contamination. We also do not have contracts with many of these suppliers, and we may not be able to contract with them on acceptable terms or at all. Accordingly, we may experience delays in receiving key raw materials to support clinical or commercial manufacturing.
In addition, some raw materials utilized in the manufacture of our candidates are currently available from a single supplier, or a small number of suppliers. For example, principal suppliers for the purchase of equipment and reagents critical for the manufacture of our product candidates include Cytiva (Global Life Sciences Solutions Operations UK Ltd), Wilson Wolf Manufacturing Corporation, Phoenix Labs, Nova Biologics, Inc., Sexton Biotechnologies and other suppliers. We cannot be sure that these suppliers will remain in business or that they will not be purchased by one of our competitors or another company that is not interested in continuing to produce these materials for our intended purpose. In addition, the lead time needed to establish a relationship with a new supplier can be lengthy, and we may experience delays in meeting demand in the event that we must switch to a new supplier. The time and effort to qualify a new supplier could result in additional costs, diversion of resources or reduced manufacturing yields, any of which would negatively impact our operating results. Further, we may be unable to enter into agreements with a new supplier on commercially reasonable terms, which could have a material adverse impact on our business.
| 23 |
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any products that we may develop.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical trials and will face an even greater risk if we commercially sell any products that we may develop. If we cannot successfully defend ourselves against claims that our product candidates or products caused injuries, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
| ● | reduced resources of our management to pursue our business strategy; | |
| ● | decreased demand for any product candidates or products that we may develop; | |
| ● | injury to our reputation and significant negative media attention; | |
| ● | withdrawal of clinical trial participants; | |
| ● | initiation of investigations by regulators; | |
| ● | product recalls, withdrawals or labelling, marketing or promotional restrictions; | |
| ● | significant costs to defend the resulting litigation; | |
| ● | substantial monetary awards paid to clinical trial participants or patients; | |
| ● | loss of revenue; and | |
| ● | the inability to commercialize any products that we may develop. |
We currently hold £5.0 million in clinical study liability annual insurance cover for each clinical study, with a per patient limit of £5.0 million, which may not be adequate to cover all liabilities that we may incur. We may need to increase our insurance coverage as we expand our clinical trials or if we commence commercialization of our product candidates. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
Risks Related to Governmental Regulations
Changes and uncertainties in the tax system in the countries in which we have operations could materially adversely affect our financial condition and results of operations, and reduce net returns to our shareholders.
We conduct business and file income tax returns in multiple jurisdictions. Our consolidated effective income tax rate could be materially adversely affected by several factors, including: changing tax laws, regulations and treaties, or the interpretation thereof; tax policy initiatives and reforms under consideration (such as those related to the Organization for Economic Co-Operation and Development’s, or OECD, Base Erosion and Profit Shifting, or BEPS, Project, the European Commission’s state aid investigations and other initiatives); the practices of tax authorities in jurisdictions in which we operate; the resolution of issues arising from tax audits or examinations and any related interest or penalties. Such changes may include (but are not limited to) the taxation of operating income, investment income, dividends received or (in the specific context of withholding tax) dividends paid.
We are unable to predict what tax reform may be proposed or enacted in the future or what effect such changes would have on our business, but such changes, to the extent they are brought into tax legislation, regulations, policies or practices in jurisdictions in which we operate, could increase the estimated tax liability that we have expensed to date and paid or accrued on our balance sheets, and otherwise affect our financial position, future results of operations, cash flows in a particular period and overall or effective tax rates in the future in countries where we have operations, reduce post-tax returns to our shareholders and increase the complexity, burden and cost of tax compliance.
| 24 |
Changes in our business strategy or operations may result in grant income being repaid to government grant awarding bodies
We have been awarded and received grant income from government agencies with respect to a number of research and development programs totaling £5.6 million since incorporation through December 31, 2021. In some cases, the grant award contains commitments for the business that extend beyond the specific program period. If the Company changes strategy or the nature of its operations, some grant awarding bodies may view this as a breach of the original terms of the grant and all or part of the original grant award may become subject to repayment. In the event of our having to return funds under prior grant awards, the Company may be required to repay up to an aggregate of £5.6 million.
Tax authorities may disagree with our positions and conclusions regarding certain tax positions, or may apply existing rules in an unforeseen manner, resulting in unanticipated costs, taxes or non-realization of expected benefits.
A tax authority may disagree with tax positions that we have taken, which could result in increased tax liabilities. For example, Her Majesty’s Revenue & Customs, or HMRC, the United States Internal Revenue Service, the IRS, or another tax authority could challenge our allocation of income by tax jurisdiction and the amounts paid between our affiliated companies pursuant to our intercompany arrangements and transfer pricing policies, including amounts paid with respect to our intellectual property development. Similarly, a tax authority could assert that we are subject to tax in a jurisdiction where we believe we have not established a taxable connection, often referred to as a “permanent establishment” under international tax treaties, and such an assertion, if successful, could increase our expected tax liability in one or more jurisdictions.
A tax authority may take the position that material income tax liabilities, interest and penalties are payable by us, for example where there has been a technical violation of contradictory laws and regulations that are relatively new and have not been subject to extensive review or interpretation, in which case we expect that we might contest such assessment. High-profile companies can be particularly vulnerable to aggressive application of unclear requirements. Many companies must negotiate their tax bills with tax inspectors who may demand higher taxes than applicable law appears to provide. Contesting such an assessment may be lengthy and costly and if we were unsuccessful in disputing the assessment, the implications could increase our anticipated effective tax rate, where applicable.
We may be unable to use net operating loss and tax credit carryforwards and certain built-in losses to reduce future tax payments or benefit from favorable UK tax legislation.
As a UK incorporated and tax resident entity, we are subject to UK corporate taxation. Due to the nature of our business, we have generated losses since inception and therefore have not paid any UK corporation tax. As of December 31, 2021, we had cumulative carryforward tax trading losses of £14.3 million. Subject to any relevant utilization criteria and restrictions (including those that limit the percentage of profits that can be reduced by carried forward losses and those that can restrict the use of carried forward losses where there is a change of ownership of more than half of our ordinary shares (including those represented by the ADSs) and a major change in the nature, conduct or scale of the trade), we expect these to be eligible for carry forward and utilization against future operating profits. The use of loss carryforwards in relation to UK profits incurred on or after April 1, 2017 are limited each year to £5.0 million per group plus, broadly, an incremental 50% of UK taxable profits.
As a company that carries out extensive research and development activities, we seek to benefit from the UK research and development tax relief programs, being the Small and Medium-sized Enterprises R&D tax relief program, or SME Program, and, to the extent that our projects are grant funded or relate to work subcontracted to us by third parties, the Research and Development Expenditure Credit program, or RDEC Program. Under the SME Program, we may be able to surrender the trading losses that arise from our qualifying research and development activities for a cash rebate of up to 14.5% of such qualifying research and development expenditures. The majority of our research, clinical trials management and manufacturing development activities are eligible for inclusion within these tax credit cash rebate claims. We may not be able to continue to claim payable research and development tax credits in the future if we cease to qualify as a SME, based on size criteria concerning employee headcount, turnover and gross assets.
We may benefit in the future from the UK’s “patent box” regime, which allows certain profits attributable to revenue from patented products (and other qualifying income) to be taxed at an effective rate of 10% by giving an additional tax deduction. We own several patents which cover our investigational therapies, and accordingly, future upfront fees, milestone fees, product revenue and royalties could be eligible for this deduction. When taken in combination with the enhanced relief available on our research and development expenditures, we expect a long-term rate of corporation tax lower than the statutory to apply to us. If, however, there are unexpected adverse changes to the UK research and development tax credit regime or the “patent box” regime, or for any reason we are unable to qualify for such advantageous tax legislation, or we are unable to use net operating loss and tax credit carryforwards and certain built-in losses to reduce future tax payments then our business, results of operations and financial condition may be adversely affected. This may impact our ongoing requirement for investment and the timeframes within which additional investment is required.
| 25 |
Failure to comply with United States health and data protection laws and regulations could lead to enforcement actions, including civil or criminal penalties, private litigation, and adverse publicity and could negatively affect our operating results and business.
We and any potential collaborators are subject to data protection laws and regulations, such as laws and regulations that address privacy and data security. In the United States, numerous federal and state laws and regulations, including state data breach notification laws, state health information privacy laws, and federal and state consumer protection laws, govern the collection, use, disclosure, and protection of health-related and other personal information. In addition, we may obtain health information from third parties, including research institutions from which we obtain clinical trial data, which are subject to privacy and security requirements under HIPAA, as amended by HITECH. To the extent that we act as a business associate to a healthcare provider engaging in electronic transactions, we may also be subject to the privacy and security provisions of HIPAA, as amended by HITECH, which restricts the use and disclosure of patient-identifiable health information, mandates the adoption of standards relating to the privacy and security of patient-identifiable health information, and requires the reporting of certain security breaches to healthcare provider customers with respect to such information. Additionally, many states have enacted similar laws that may impose more stringent requirements on entities like ours. Depending on the facts and circumstances, we could be subject to significant civil, criminal, and administrative penalties if we obtain, use, or disclose individually identifiable health information maintained by a HIPAA-covered entity in a manner that is not authorized or permitted by HIPAA.
Additionally, in June 2018, the State of California enacted the California Consumer Privacy Act of 2018, or CCPA, which came into effect on January 1, 2020 and provides new data privacy rights for consumers (as that term is broadly defined) and new operational requirements for companies, which may increase our compliance costs and potential liability. The CCPA gives California residents expanded rights to access and delete their personal information, opt out of certain personal information sharing, and receive detailed information about how their personal information is used. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches that is expected to increase data breach litigation. While there is currently an exception for protected health information that is subject to HIPAA and clinical trial regulations, as currently written, the CCPA may impact certain of our business activities. The CCPA could mark the beginning of a trend toward more stringent state privacy legislation in the United States, which could increase our potential liability and adversely affect our business.
Compliance with U.S. and foreign privacy and data protection laws and regulations could require us to take on more onerous obligations in our contracts, restrict our ability to collect, use and disclose data, or in some cases, impact our ability to operate in certain jurisdictions. Failure to comply with these laws and regulations could result in government enforcement actions (which could include civil, criminal and administrative penalties), private litigation, and/or adverse publicity and could negatively affect our operating results and business. Moreover, clinical trial subjects, employees and other individuals about whom we or our potential collaborators obtain personal information, as well as the providers who share this information with us, may limit our ability to collect, use and disclose the information. Claims that we have violated individuals’ privacy rights, failed to comply with data protection laws, or breached our contractual obligations, even if we are not found liable, could be expensive and time-consuming to defend and could result in adverse publicity that could harm our business.
European data collection is governed by restrictive privacy and security regulations governing the use, processing and cross-border transfer of personal information.
The collection, use, storage, disclosure, transfer, or other processing of personal data (including health data processed in the context of clinical trials) (i) regarding individuals in the EU, and/or (ii) carried out in the context of the activities of our establishment in any EU member state, is subject to the EU General Data Protection Regulation, or GDPR, which became effective on May 25, 2018, as well as other national data protection legislation in force in relevant member states (including the Data Protection Act 2018 in the UK).
| 26 |
The GDPR is wide-ranging in scope and imposes numerous additional requirements on companies that process personal data, including imposing special requirements in respect of the processing of health and other sensitive data, requiring that consent of individuals to whom the personal data relates is obtained in certain circumstances, requiring additional disclosures to individuals regarding data processing activities, requiring that safeguards are implemented to protect the security and confidentiality of personal data, creating mandatory data breach notification requirements in certain circumstances, and requiring that certain measures (including contractual requirements) are put in place when engaging third-party processors. The GDPR also imposes strict rules on the transfer of personal data to countries outside the EEA, including the United States, and permits data protection authorities to impose large penalties for violations of the GDPR, including potential fines of up to €20 million or 4% of annual global revenue, whichever is greater. The GDPR provides individuals with various rights in respect of their personal data, including rights of access, erasure, portability, rectification, restriction and objection. The GDPR also confers a private right of action on data subjects and consumer associations to lodge complaints with supervisory authorities, seek judicial remedies, and obtain compensation for damages resulting from violations of the GDPR.
The GDPR may increase our responsibility and liability in relation to personal data that we process where such processing is subject to the GDPR. While we have taken steps to comply with the GDPR, and implementing legislation in applicable EU member states, including by seeking to establish appropriate lawful bases for the various processing activities we carry out as a controller or joint controller, reviewing our security procedures and those of our vendors and collaborators, and entering into data processing agreements with relevant vendors and collaborators, we cannot be certain that our efforts to achieve and remain in compliance have been, and/or will continue to be, fully successful.
Following the UK’s withdrawal from the EU on January 31, 2020 and following the end the of the transitional arrangements on December 31, 2020, it is likely that the data protection obligations of the GDPR will continue to apply to UK-based organizations’ processing of personal data in substantially unvaried form, for at least the short term thereafter.
Risks Related to Our Business Operations, Managing Growth and Employee Matters
We may have difficulty managing growth in our business.
Because of our small size, growth in accordance with our business plan, if achieved, will place a significant strain on our financial, technical, operational and management resources. As we expand our activities, there will be additional demands on these resources. The failure to continue to upgrade our technical, administrative, operating and financial control systems or the occurrence of unexpected expansion difficulties, including issues relating to our research and development activities and retention of experienced scientists, managers and engineers, could have a material adverse effect on our business, financial condition and results of operations and our ability to timely execute our business plan. If we are unable to implement these actions in a timely manner, our results may be adversely affected.
We depend upon our key personnel and our ability to attract and retain employees
We are heavily dependent on the ongoing employment and involvement of certain key employees. These include (i) Bryan Kobel, our Chief Executive Officer, (ii) Dr Michael Leek, our Executive Chairman of the Board, (iii) Angela Scott, our Chief Operating Officer, (iv) Martin Thorp, our Chief Financial Officer and (v) Sebastian Wanless, our Director of Clinical operations. In response to this dependence, we have and plan to maintain for a period into the future appropriate key man insurance.
Dr Michael Leek and Angela Scott are married. They are our co-founders and are a vital part of our business. If the marriage ended or they could otherwise not amicably work with each other, one of them may decide to leave us which would materially harm our business.
| 27 |
We anticipate a requirement to expand our current personnel, who will be based in the UK, the EU and the USA, very rapidly in order to achieve our planned business activities and aims to further engage in clinical trials. Such expansion is dependent on our ability to recruit experienced and suitably trained employees or consultants, and to retain such employees on a long-term basis. Our ability to take our existing pipeline of GD-T cell therapeutics and to meet the demands of our clinical programs may be compromised or delayed if we are unable to recruit sufficient personnel on a timely basis.
The loss of key managers and senior scientists could delay our research and development activities. In addition, our ability to compete in the highly competitive pharmaceutical industry depends upon our ability to attract and retain highly qualified management, scientific and medical personnel. Many other companies and academic institutions that we compete against for qualified personnel have greater financial and other resources, different risk profiles and a longer history in the industry than we do. Therefore, we might not be able to attract or retain these key persons on conditions that are economically acceptable. Moreover, some qualified prospective employees may choose not to work for us due to negative perceptions regarding the therapeutic use of psilocybin or other objections to the therapeutic use of a controlled substance. Furthermore, we will need to recruit new managers and qualified scientific personnel to develop our business if we expand into fields that will require additional skills. Our inability to attract and retain these key persons could prevent us from achieving our objectives and implementing our business strategy, which could have a material adverse effect on our business and prospects.
In addition, certain key academic and scientific personnel play a pivotal role in our collaborative partners’ research and development activities. If any of those key academic and scientific personnel who work on development of our research programs, our investigational GD-T cell therapy and any future therapeutic candidates leave our collaborative partners, the development of our research programs, our investigational GD-T cell therapy and any future therapeutic candidates may be delayed or otherwise adversely affected.
We will need to grow the size and capabilities of our organization, and we may experience difficulties in managing this growth.
As of April 30, 2022, we have 76 full-time equivalent employees. As our development and commercialization plans and strategies develop, and as we transition into operating as a public company, we will have to add a significant number of additional managerial, operational, financial, and other personnel. Future growth will impose significant added responsibilities on members of management, including:
| ● | identifying, recruiting, integrating, maintaining, and motivating additional employees; | |
| ● | managing our internal development efforts effectively, including the clinical and regulatory review process for our GD-T therapeutic candidates, while complying with our contractual obligations to contractors and other third parties; and | |
| ● | improving our operational, financial and management controls, reporting systems, and procedures. |
Our future financial performance and our ability to commercialize our GD-T therapeutic candidates will depend, in part, on our ability to effectively manage any future growth, and our management may also have to divert a disproportionate amount of its attention away from day-to-day activities in order to devote a substantial amount of time to managing these growth activities.
If we fail to maintain proper and effective internal controls, our ability to produce accurate financial statements on a timely basis could be impaired, which would adversely affect our business and our stock price.
Ensuring that we have adequate internal financial and accounting controls and procedures in place to produce accurate financial statements on a timely basis is a costly and time-consuming effort that needs to be re-evaluated frequently. We may discover material weaknesses in our internal financial and accounting controls and procedures that need improvement from time to time.
Management is responsible for establishing and maintaining adequate internal control over financial reporting to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of financial statements for external purposes. Management does not expect that our internal control over financial reporting will prevent or detect all errors and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that misstatements due to error or fraud will not occur or that all control issues and instances of fraud, if any, within our company will have been detected.
| 28 |
Pursuant to Section 404 of the Sarbanes-Oxley Act of 2002, or Section 404, we are required to furnish a report by our senior management on our internal control over financial reporting, commencing with our second annual report. However, while we remain an EGC we are not required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To prepare for eventual compliance with Section 404, once we no longer qualify as an EGC, we are engaged in a process to document and evaluate our internal control over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, potentially engage outside consultants, adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented, and implement a continuous reporting and improvement process for internal control over financial reporting. Despite our efforts, there is a risk that we will not be able to conclude, within the prescribed timeframe or at all, that our internal control over financial reporting is effective as required by Section 404. If we identify one or more material weaknesses, it could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements. In addition, if we are unable to produce accurate financial statements on a timely basis, investors could lose confidence in the reliability of our financial statements, which could cause the market price of either of our ADSs or Warrants, or both, to decline and make it more difficult for us to finance our operations and growth.
A pandemic, epidemic, or outbreak of an infectious disease, such as the COVID-19 pandemic, may materially and adversely affect our business, including our preclinical studies, clinical trials, third parties on whom we rely, our supply chain, our ability to raise capital, our ability to conduct regular business and our financial results.
We are subject to risks related to public health crises such as the COVID-19 pandemic. The COVID-19 pandemic continues throughout the world. The pandemic and policies and regulations implemented by governments in response to the pandemic, often directing businesses and governmental agencies to cease non-essential operations at physical locations, prohibiting certain nonessential gatherings and ceasing non-essential travel have also had a significant impact, both direct and indirect, on businesses and commerce, as worker shortages have occurred, supply chains have been disrupted, facilities and production have been suspended, and demand for certain goods and services, such as medical service and supplies, has spiked, while demand for other goods and services, such as travel, has fallen. The full extent to which COVID-19 will ultimately impact our business, preclinical trials and financial results will depend on future developments, which are highly uncertain and cannot be accurately predicted, including new information which may emerge concerning the severity of COVID-19 and the actions to contain COVID-19 or treat its impact, among others. Global health concerns, such as the COVID-19 pandemic, could also result in social, economic, and labor instability in the countries in which we or the third parties with whom we engage operate.
In response to the COVID-19 pandemic, we have taken temporary precautionary measures intended to help minimize the risk of the virus to our employees, including flexibility for employees to work remotely where appropriate, suspending all non-essential travel worldwide for our employees and discouraging employee attendance at industry events and in-person work-related meetings, all of which could negatively affect our business. The extent of the impact of the COVID-19 pandemic on our preclinical studies or clinical trial operations, our supply chain and manufacturing and our office-based business operations, will depend on future developments, which are highly uncertain and cannot be predicted with confidence, such as the duration of the pandemic, the severity of the COVID-19 pandemic, or the effectiveness of actions to contain and treat coronavirus.
While we are working closely with our third-party manufacturers, distributors and other partners to manage our supply chain activities and mitigate potential disruptions to current and any future therapeutic candidates as a result of the COVID-19 pandemic, if the COVID-19 pandemic continues and persists for an extended period of time, we expect there will be significant and material disruptions to our supply chain and operations, and associated delays in the manufacturing and supply of current and any future therapeutic candidates. Any such supply disruptions would adversely impact our ability to generate sales of and revenue from our approved products and our business, financial condition, results of operations and growth prospects could be materially adversely affected.
The COVID-19 pandemic may also affect employees of third-party CROs located in affected geographies that we rely upon to carry out our clinical trials. As COVID-19 continues to be present and spread around the globe, we may experience additional disruptions that could severely impact our business and clinical trials, including:
| ● | delays or difficulties in enrolling patients in our clinical trials; |
| 29 |
| ● | delays or difficulties in clinical site initiation, including difficulties in recruiting clinical site investigators and clinical site staff; | |
| ● | diversion of healthcare resources away from the conduct of clinical trials, including the diversion of sites or facilities serving as our clinical trial sites and staff supporting the conduct of our clinical trials, including our trained therapists, or absenteeism due to the COVID-19 pandemic that reduces site resources; | |
| ● | interruption of key clinical trial activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal, state or national governments, employers and others or interruption of clinical trial subject visits and study procedures, the occurrence of which could affect the integrity of clinical trial data; | |
| ● | risk that participants enrolled in our clinical trials will acquire COVID-19 while the clinical trial is ongoing, which could impact the results of the clinical trial, including by increasing the number of observed adverse events or patient withdrawals from our trials; | |
| ● | limitations in employee resources that would otherwise be focused on conducting our clinical trials, including because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; | |
| ● | delays in receiving authorizations from regulatory authorities to initiate our planned clinical trials; | |
| ● | delays in clinical sites receiving the supplies and materials needed to conduct our clinical trials; | |
| ● | interruption in global shipping that may affect the transport of clinical trial materials, such as the cell therapy used in our clinical trials; | |
| ● | changes in local regulations as part of a response to the COVID-19 pandemic which may require us to change the ways in which our clinical trials are conducted, which may result in unexpected costs, or the discontinuation of the clinical trials altogether; | |
| ● | interruptions or delays in preclinical studies due to restricted or limited operations at research and development laboratory facilities; | |
| ● | delays in necessary interactions with local regulators, ethics committees and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; and | |
| ● | refusal of the FDA, the EMA, the MHRA or the other regulatory bodies to accept data from clinical trials in affected geographies outside the United States or the EU or other relevant local geography. |
Any negative impact the COVID-19 pandemic has on patient enrolment or treatment or the development of our investigational cell therapies and any future therapeutic candidates could cause costly delays to clinical trial activities, which could adversely affect our ability to obtain regulatory approval for and to commercialize our investigational cell therapies and any future therapeutic candidates, if approved, increase our operating expenses, and have a material adverse effect on our financial results.
The COVID-19 pandemic has also caused significant volatility in public equity markets and disruptions to the United States and global economies. This increased volatility and economic dislocation may make it more difficult for us to raise capital on favorable terms, or at all. We cannot currently predict the scope and severity of any potential business shutdowns or disruptions. If we or any of the third parties with whom we engage, however, were to experience shutdowns or other business disruptions, our ability to conduct our business in the manner and on the timelines presently planned could be materially and negatively affected, which could have a material adverse impact on our business and our results of operations and financial conditions. To the extent the COVID-19 pandemic adversely affects our business and financial results, it may also heighten many of the other risks described in this “Risk Factors” section, such as those relating to the timing and completion of our clinical trials and our ability to obtain future financing.
| 30 |
Our current operations are headquartered in one location, and we or the third parties upon whom we depend may be adversely affected by unplanned natural disasters, as well as occurrences of civil unrest, and our business continuity and disaster recovery plans may not adequately protect us from a serious disaster, including earthquakes, outbreak of disease or other natural disasters.
Our current business operations are headquartered in our offices in Glasgow, UK, with an additional office in Leiden in the Netherlands. Any unplanned event, such as flood, fire, explosion, earthquake, extreme weather condition, medical epidemics, power shortage, telecommunication failure or other natural or man-made accidents or incidents, including events of civil unrest that result in us being unable to fully utilize our facilities, or the manufacturing facilities of our third-party contract manufacturers, may have a material and adverse effect on our ability to operate our business, particularly on a daily basis, and have significant negative consequences on our financial and operating conditions. Loss of access to these facilities may result in increased costs, delays in the development of our investigational GD-T cell therapy or any future therapeutic candidates or interruption of our business operations.
The disaster recovery and business continuity plans we have in place may prove inadequate in the event of a serious disaster or similar event. We may incur substantial expenses as a result of the limited nature of our disaster recovery and business continuity plans, which, could have a material adverse effect on our business. As part of our risk management policy, we maintain insurance coverage at levels that we believe are appropriate for our business, but in the final result may not be sufficient to satisfy any damages and losses.
The increasing use of social media platforms presents new risks and challenges.
Social media is increasingly being used to communicate about our clinical development programs and the diseases our investigational GD-T cell therapy or any future therapeutic candidates are being developed to treat, and we may use appropriate social media in connection with our commercialization efforts of our investigational GD-T cell therapy following approval of our GD-T cell therapy or any future therapeutic candidates, if any. Social media practices in the biopharmaceutical industry continue to evolve, and regulations and regulatory guidance relating to such use are evolving and not always clear. This evolution creates uncertainty and risk of noncompliance with regulations applicable to our business, resulting in potential regulatory actions against us, along with the potential for litigation related to certain prohibited activities. For example, patients may use social media channels to comment on their experience in an ongoing clinical trial or to report an alleged adverse event. When such disclosures occur, there is a risk that trial enrolment may be adversely impacted, we fail to monitor and comply with applicable adverse event reporting obligations, or that we may not be able to defend our business or the public’s legitimate interests in the face of the political and market pressures generated by social media due to restrictions on what we may say about our investigational GD-T cell therapy or any future therapeutic candidates. There is also a risk of inappropriate disclosure of sensitive information or negative or inaccurate posts or comments about us on any social networking website. If any of these events were to occur or we otherwise fail to comply with applicable regulations, we could incur liability, face regulatory actions or incur other harm to our business.
Risks Related to Intellectual Property
If we or our licensors are unable to protect our/their intellectual property, then our financial condition, results of operations and the value of our drug technology and product candidates could be adversely affected.
Patents and other proprietary rights are essential to our business, and our ability to compete effectively with other companies is dependent upon the proprietary nature of our drug technologies and product candidates. We also rely upon trade secrets, know-how, continuing innovations and licensing opportunities to develop, maintain and strengthen our competitive position. We seek to protect these, in part, through confidentiality agreements with employees, consultants and other parties. Our success will depend in part on the ability of TCB and our licensors to obtain, to maintain (including making periodic filings and payments) and to enforce patent protection for the licensed intellectual property, in particular, those patents to which we have secured rights. We, and our licensors, may not successfully prosecute or continue to prosecute the patent applications which we have licensed. Even if patents are issued in respect of these patent applications, TCB or our licensors may fail to maintain these patents, may determine not to pursue litigation against entities that are infringing upon these patents, or may pursue such enforcement less aggressively than we ordinarily would for our own patents. Without adequate protection for the intellectual property that we own or license, other companies might be able to offer substantially identical products for sale, which could unfavorably affect our competitive business position and harm our business prospects. Even if issued, patents may be challenged, invalidated, or circumvented, which could limit our ability to stop competitors from marketing similar products or limit the length of term of patent protection that we may have for our products.
| 31 |
Litigation or third-party claims of intellectual property infringement or challenges to the validity of our patents would require us to use resources to protect our rights and may prevent or delay our development, regulatory approval or commercialization of our product candidates.
If we are the target of claims by third parties asserting that our product candidates and products or intellectual property infringe upon the rights of others we may be forced to incur substantial expenses or divert substantial employee resources from our current business endeavors. If successful, those claims could result in our having to pay substantial damages or could prevent us from developing one or more product candidates or commercializing a product. Further, if a patent infringement suit were brought against us or our collaborators, we or they could be forced to stop or delay research, development, manufacturing or sales of the product candidate or product that is the subject of the suit.
If we or our collaborators experience patent infringement claims, or if we elect to avoid potential claims others may be able to assert, we or our collaborators may choose to seek, or be required to seek, a license from the third-party and would most likely be required to pay license fees or royalties or both. These licenses may not be available on acceptable terms, or at all. Even if we or our collaborators were able to obtain a license, the rights may be nonexclusive, which would give our competitors access to the same intellectual property. Ultimately, we could be prevented from commercializing a product, or be forced to cease some aspect of our business operations if, as a result of actual or threatened patent infringement claims, we or our collaborators are unable to enter into licenses on acceptable terms. This could harm our business significantly. The cost to us of any litigation or other proceeding, regardless of its merit, even if resolved in our favor, could be substantial. Some of our competitors may be able to bear the costs of such litigation or proceedings more effectively than we can because of their having greater financial resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace. Intellectual property litigation and other proceedings may, regardless of their merit, also absorb significant management time and employee resources.
If we are unable to obtain and maintain patent protection for our GD-T cell technologies and product candidates, or if the scope of the patent protection obtained is not sufficiently broad, our competitors could develop and commercialize technology and biologics similar or identical to ours, and our ability to successfully commercialize our technology and product candidates may be impaired.
Our success depends on our ability to obtain and maintain patent protection in the United States, the European Union, Japan and other countries with respect to our product candidates. We seek to protect our proprietary position by filing patent applications related to our technology and product candidates in the major pharmaceutical markets, including the United States, major countries in Europe and Japan. If we do not adequately protect our intellectual property, competitors may be able to use our technologies and erode or negate any competitive advantage that we may have, which could harm our business and ability to achieve profitability.
To protect our proprietary positions, we file patent applications related to our novel technologies and product candidates that are important to our business. The patent application and prosecution process is expensive and time-consuming. We may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. We may also fail to identify patentable aspects of our research and development before it is too late to obtain patent protection. It is possible that defects of form in the preparation or filing of our patents or patent applications may exist, or may arise in the future, such as with respect to proper priority claims, inventorship, claim scope or patent term adjustments. If any current or future licensors or licensees are not fully cooperative or disagree with us as to the prosecution, maintenance or enforcement of any patent rights, such patent rights could be compromised and we might not be able to prevent third parties from making, using and selling competing products. If there are material defects in the form or preparation of our patents or patent applications, such patents or applications may be invalid and unenforceable. Moreover, our competitors may independently develop equivalent knowledge, methods and know-how. Any of these outcomes could impair our ability to prevent competition from third parties.
| 32 |
Patent applications are generally in the form of composition of matter or method patents. A composition of matter (COM) patent protects an actual drug molecule or engineered cell or other therapeutic agent and will be infringed by a third party making any use of the protected composition. COM patents provide de-facto protection for any and all uses of the protected composition and are generally held to be the strongest and most valuable form of patent protection. Method patents protect, for example, a method of manufacturing a product or a method of using it. They can be valuable but typically are more limited in scope than COM patents, particularly method of use patents which only protect a particular application of a product. Where our patent applications are limited in their scope, such as a patent protecting the method of use, such patent rights could be compromised and we might not be able to prevent third parties from making, using and selling competing products.
Prosecution of our owned and in-licensed patent portfolio is at a very early stage. We have one granted US patent, one granted Australian patent and one granted Israeli patent to date and no granted European patents. Most of our current patent portfolio consists of applications pending at a number of national or regional patent offices (Australia, Canada, Brazil, China, Eurasia, Europe, Hong Kong, Israel, Japan, South Korea, New Zealand, Singapore, US, South Africa). Neither priority applications nor PCT applications can themselves give rise to issued patents. Rather, protection for the inventions disclosed in these applications must be further pursued by applicable deadlines via applications that are subject to examination. As applicable deadlines for the priority and PCT applications become due, we will need to decide whether to and in which countries or jurisdictions to pursue patent protection for the various inventions claimed in these applications, and we will only have the opportunity to pursue and obtain patents in those jurisdictions where we pursue protection.
It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. The patent applications that we own or in-license may fail to result in issued patents with claims that cover our current and future product candidates in the countries in which we pursue patent protection. Our patent applications cannot be enforced against third parties practicing the technology claimed in such applications unless, and until, a patent issues from such applications, and then only to the extent the issued claims cover the technology.
If the patent applications we hold or have in-licensed with respect to our development programs and product candidates fail to issue, if their breadth or strength of protection is threatened, or if they fail to provide meaningful exclusivity for our current and future product candidates, it could threaten our ability to commercialize our product candidates. Any such outcome could have a negative effect on our business.
Patent and other intellectual property rights may not be upheld, in which case we will suffer a loss of our intellectual property position and the value of our assets.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain. Changes in either the patent laws or interpretation of the patent laws of the various jurisdictions in which we pursue patents may diminish the value of our patents or narrow the scope of our patent protection. In addition, the protections offered by laws of different countries vary. No consistent policy regarding the breadth of claims allowed in biotechnology and pharmaceutical patents has emerged to date in many jurisdictions. In addition, the determination of patent rights with respect to pharmaceutical technologies, such as our cell technologies, commonly involves complex legal and factual questions, which has in recent years been the subject of much litigation. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights, whether owned or in-licensed, are highly uncertain. Furthermore, the scope, strength and enforceability of our patent rights or the nature of proceedings that may be brought by or against us related to our patent rights may change as the related patent and intellectual property laws change over time. Additionally, in the United States, one of the jurisdictions in which we purse patent protection, the U.S. Supreme Court has ruled on several patent cases in recent years either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on decisions by the U.S. Congress, the U.S. federal courts, and the USPTO, the laws and regulations governing patents could change in unpredictable ways that could weaken our ability to obtain patents or to enforce any patents that we might obtain in the future.
| 33 |
We may be unaware of the rights of others which may ultimately be used to limit our intellectual property rights.
We may not be aware of all third-party intellectual property rights potentially relating to our current and future our product candidates. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in many jurisdictions typically are not published until 18 months or more after filing, or in some cases not at all. Therefore, we cannot be certain that we or our licensors were the first to make the inventions claimed in our patents or pending patent applications, or that we or our licensors were the first to file for patent protection of such inventions. Similarly, should we own or in-license any patents or patent applications in the future, we may not be certain that we or the applicable licensor were the first to file for patent protection for the inventions claimed in such patents or patent applications. As a result, the issuance, scope, validity and commercial value of our patent rights cannot be predicted with any certainty. Moreover, in the United States, we may be subject to a third-party pre-issuance submission of prior art to the U.S. Patent and Trademark Office, or USPTO, or become involved in opposition, derivation, re-examination, inter partes review or interference proceedings, in the United States or elsewhere, challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our technology or product candidates and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights, which could significantly harm our business and results of operations.
We may be subject to claims by third parties asserting that we or our employees have misappropriated their intellectual property, or claiming ownership of what we regard as our own intellectual property.
Many of our employees were previously employed at universities or other biotechnology or pharmaceutical companies. Although we try to ensure that our employees do not use the proprietary information or know-how of third parties in their work for us, we may be subject to claims that these employees or we have inadvertently or otherwise used intellectual property, including trade secrets or other proprietary information, of any such employee’s former employer. We may also in the future be subject to claims that we have caused an employee to breach the terms of his or her non-competition or non-solicitation agreement. Litigation may be necessary to defend against these potential claims.
In addition, while it is our policy to require our employees and contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, such employees and contractors may breach the agreement and claim the developed intellectual property as their own.
If we fail in defending any the claims we have made, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. A court could prohibit us from using technologies or features that are essential to our products if such technologies or features are found to incorporate or be derived from the trade secrets or other proprietary information of the former employers. Even if we are successful in prosecuting or defending against such claims, litigation could result in substantial costs and could be a distraction to management. In addition, any litigation or threat thereof may adversely affect our ability to hire employees or contract with independent service providers. Moreover, a loss of key personnel or their work product could hamper or prevent our ability to commercialize our products.
Technologies and other proprietary rights for which we seek patent protection may not be obtained, which would potentially limit the value of our intellectual property.
Our pending and future patent applications, whether owned or in-licensed, may not result in patents being issued that protect our technology or product candidates, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products. Even if our patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection against competing products or processes sufficient to achieve our business objectives, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our owned or licensed patents, should they issue, by developing similar or alternative technologies or products in a non-infringing manner. Our competitors may seek approval to market their own products similar to or otherwise competitive with our products. In these circumstances, we may need to defend and/or assert our patents, including by filing lawsuits alleging patent infringement. In any of these types of proceedings, a court or other agency with jurisdiction may find our patents invalid and/or unenforceable.
| 34 |
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our owned and licensed patents may be challenged in the courts or patent offices in the jurisdictions in which we have filed for patent protection. Such challenges may result in loss of exclusivity or freedom to operate or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. In addition, given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized.
We may be subject to claims challenging the inventorship or ownership of our owned or in-licensed patent rights and other intellectual property.
We generally enter into confidentiality and intellectual property assignment agreements with our employees, consultants, outside scientific collaborators, sponsored researchers and other advisors. However, these agreements may not be honored and may not effectively assign intellectual property rights to us. For example, disputes may arise from conflicting obligations of consultants or others who are involved in developing our technology and product candidates. Litigation may be necessary to defend against these and other claims challenging inventorship or ownership. The owners of intellectual property in-licensed to us could also face such claims. If we or our licensors fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Such an outcome could have a material adverse effect on our business. Even if we or our licensors are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Third parties may initiate legal proceedings alleging that we are infringing their intellectual property rights, the outcome of which would be uncertain and could significantly harm our business.
We believe that we have proprietary and modular T cell programming technology that does not infringe the intellectual property and other proprietary rights of third parties. Numerous third-party U.S. and non-U.S. issued patents exist in the area of biotechnology, including in the area of programmed T cell therapies. Some are patents held by our competitors. If any third-party patents cover our product candidates or technologies, we may not be free to manufacture or commercialize our product candidates as planned.
There is a substantial amount of intellectual property litigation in the biotechnology and pharmaceutical industries, and we may become party to, or threatened with, litigation or other adversarial proceedings regarding intellectual property rights with respect to our technology or product candidates, including interference proceedings before the relevant patent office. Intellectual property disputes arise in a number of areas including with respect to patents, use of other proprietary rights and the contractual terms of license arrangements. Third parties may assert claims against us based on existing or future intellectual property rights and claims may also come from competitors against whom our own patent portfolio may have no deterrent effect. The outcome of intellectual property litigation is subject to uncertainties that cannot be adequately quantified in advance. Other parties may allege that our product candidates or the use of our technologies infringes patent claims or other intellectual property rights held by them or that we are employing their proprietary technology without authorization. As we continue to develop and, if approved, commercialize our current and future product candidates, competitors may claim that our technology infringes their intellectual property rights as part of business strategies designed to impede our successful commercialization. There are and may in the future be additional third-party patents or patent applications with claims to, for example, materials, compositions, formulations, methods of manufacture or methods for treatment related to the use or manufacture of any one or more of our product candidates.
If we are found to infringe a third party’s intellectual property rights, we could be forced, including by court order, to cease developing, manufacturing or commercializing the infringing product candidate or product. Alternatively, we may be required or may choose to obtain a license from such third party in order to use the infringing technology and continue developing, manufacturing or marketing the infringing product candidate. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if we were able to obtain a license, it could be non-exclusive, thereby giving our competitors access to the same technologies licensed to us. In addition, we could be found liable for monetary damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent. A finding of infringement could prevent us from commercializing our product candidates or force us to cease some of our business operations. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative effect on our business. Even if successful, the defense of any claim of infringement or misappropriation is time-consuming, expensive and diverts the attention of our management from our ongoing business operations.
| 35 |
We may need to license intellectual property from third parties, and such licenses may not be available or may not be available on commercially reasonable terms.
A third party may hold intellectual property rights, including patent rights, which are important or necessary to the development or manufacture of our product candidates. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our product candidates, in which case we would be required to obtain a license from these third parties. Such a license may not be available on commercially reasonable terms, or at all, and we could be forced to accept unfavorable contractual terms. If we are unable to obtain such licenses on commercially reasonable terms, our business could be harmed.
We may become involved in lawsuits to protect or enforce our intellectual property, which could be expensive, time-consuming and unsuccessful.
Competitors may infringe our patents, if issued, trademarks, copyrights or other intellectual property. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming and divert the time and attention of our management and scientific personnel. Any claims we assert against perceived infringers could provoke these parties to assert counterclaims against us alleging that we infringe their patents, trademarks, copyrights or other intellectual property. In addition, in a patent infringement proceeding, there is a risk that a court will decide that a patent of ours is invalid or unenforceable, in whole or in part, and that we do not have the right to stop the other party from using the invention at issue. There is also a risk that, even if the validity of such patents is upheld, the court will construe the patent’s claims narrowly or decide that we do not have the right to stop the other party from using the invention at issue on the grounds that our patents do not cover the invention. An adverse outcome in a litigation or proceeding involving our patents could limit our ability to assert our patents against those parties or other competitors, and may curtail or preclude our ability to exclude third parties from making and selling similar or competitive products. Similarly, if we assert trademark infringement claims, a court may determine that the marks we have asserted are invalid or unenforceable, or that the party against whom we have asserted trademark infringement has superior rights to the marks in question. In this case, we could ultimately be forced to cease use of such trademarks.
In any infringement litigation, any award of monetary damages we receive may not be commercially valuable. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during litigation. Moreover, there can be no assurance that we will have sufficient financial or other resources to file and pursue such infringement claims, which typically last for years before they are concluded. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources and more mature and developed intellectual property portfolios. Even if we ultimately prevail in such claims, the monetary cost of such litigation and the diversion of the attention of our management and scientific personnel could outweigh any benefit we receive as a result of the proceedings. Accordingly, despite our efforts, we may not be able to prevent third parties from infringing, misappropriating or successfully challenging our intellectual property rights. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a negative impact on our ability to compete in the marketplace.
Any trademarks we may obtain may be infringed or successfully challenged, resulting in harm to our business.
We expect to rely on trademarks as one means to distinguish any of our product candidates that are approved for marketing from the products of our competitors. While we have a corporate trademark, we have not yet selected trademarks for our product candidates and have not yet begun the process of applying to register trademarks for our product candidates. Once we select trademarks and apply to register them, our trademark applications may not be approved. Third parties may oppose our trademark applications, or otherwise challenge our use of the trademarks. In the event that our trademarks are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition and could require us to devote resources to advertising and marketing new brands. Our competitors may infringe our trademarks and we may not have adequate resources to enforce our trademarks.
| 36 |
In addition, any proprietary name we propose to use with our clinical-stage product candidates or any other product candidate in the United States must be approved by the FDA, regardless of whether we have registered it, or applied to register it, as a trademark. The FDA typically conducts a review of proposed product names, including an evaluation of the potential for confusion with other product names. If the FDA objects to any of our proposed proprietary product names, we may be required to expend significant additional resources in an effort to identify a suitable proprietary product name that would qualify under applicable trademark laws, not infringe the existing rights of third parties and be acceptable to the FDA.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition to seeking patent and trademark protection for our product candidates, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive position. We seek to protect our trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, consultants, advisors and other third parties. We also enter into confidentiality and invention or patent assignment agreements with our employees and consultants. Despite these efforts, any of these parties may breach the agreements and disclose our proprietary information, including our trade secrets. Monitoring unauthorized uses and disclosures of our intellectual property is difficult, and we do not know whether the steps we have taken to protect our intellectual property will be effective. In addition, we may not be able to obtain adequate remedies for any such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts in the jurisdiction in which we operate or intend to operate are less willing or unwilling to protect trade secrets.
Moreover, our competitors may independently develop knowledge, methods and know-how equivalent to our trade secrets. Competitors could purchase our products and replicate some or all of the competitive advantages we derive from our development efforts for technologies on which we do not have patent protection. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance and annuity fees on any issued patent are due to be paid to the patent offices and patent agencies over the lifetime of the patent to maintain the patents that have been issued. Additionally, these offices and agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Non-compliance events that could result in abandonment or lapse of a patent or patent application include failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we or our licensors fail to maintain the patents and patent applications covering our products or product candidates, our competitors might be able to enter the market, which would harm our business. In addition, to the extent that we have responsibility for taking any action related to the prosecution or maintenance of patents or patent application in-licensed from a third party, any failure on our part to maintain the in-licensed rights could jeopardize our rights under the relevant license and may expose us to liability.
| 37 |
If we fail to comply with our obligations in the agreements under which we license our development or commercialization rights to products or drug technologies from third parties, we could lose license rights that are important to our business.
We hold a license from UCL Business plc (“UCLB”) for its technology related to co-stimulatory CAR-T in GD-T cells. This is in addition to the intellectual property that we own. Our license with UCLB is for a single CAR-T binder, where we pay an annual license fee, certain performance-based milestone payments and a single-digit royalty on sales arising from use of that binder together with certain cumulative sales-based milestone payments. Through December 31, 2021 we have paid UCLB approximately $0.5 million (taking into consideration fluctuation in exchange rates) in license fee payments. Furthermore, the Company has a duty not to breach terms of the license agreement. If we fail to meet specific obligations, the licensor will have the right to terminate the applicable license or modify certain terms of the license agreement. Royalty provisions cease upon termination or upon expiry of the license which occurs, on a country-by-country basis, upon the later of the tenth (10th) anniversary of the first commercial sale of a licensed product or the lapse, expiry, or revocation of all patents.
Risks Related Ownership of Our ADSs and Warrants
Control by a limited number of shareholders may limit the ability of investors to influence the outcome of director elections and other transactions requiring shareholder approval.
Our directors, management persons and 5% and greater shareholders, as a group, own approximately 79.9% of our issued and outstanding ordinary shares (including those represented by the ADSs), including options and other convertible securities that may be converted within sixty days of March 1, 2022. The foregoing percentage calculation does not take into account any of the public warrants. Dr. Michael Leek and Angela Scott, who are married, our founders, and are part of our management team, own approximately 14.5% of our outstanding ordinary shares on a beneficial basis. Such persons together, along with several other long term significant shareholders, will have influence over corporate actions requiring shareholder approval, including the following actions:
| ● | to elect our directors; | |
| ● | to amend or prevent amendment of our articles of association; | |
| ● | to effect or prevent a merger, sale of assets or other corporate transaction; and | |
| ● | to influence the outcome of any other matter submitted to our shareholders for vote. |
These persons’ share ownership may discourage a potential acquirer from making a tender offer or otherwise attempting to obtain control of our company, which in turn could reduce the market price of our ADSs and Warrants or prevent our shareholders from realizing a premium over the market price of our ADSs and Warrants.
We are a foreign private issuer and, as a result, we are not subject to U.S. proxy rules and are subject to Exchange Act reporting obligations that, to some extent, are more lenient and less frequent than those of a U.S. domestic public company.
As a foreign private issuer we report under the Exchange Act as a non-U.S. company. We are exempt from certain provisions of the Exchange Act that are applicable to U.S. domestic public companies. These include: (1) the sections of the Exchange Act regulating the solicitation of proxies, consents or authorizations with respect to a security registered under the Exchange Act; (2) the Section 16 of the Exchange Act requiring insiders to file public reports of their stock ownership and trading activities and liability for insiders who profit from trades made in a short period of time; and (3) the rules under the Exchange Act requiring the filing with the SEC of quarterly reports containing unaudited financial and other specified information, or current reports upon the occurrence of specified significant events. In addition, foreign private issuers are not required to file their annual report on Form 20-F until four months after the end of each fiscal year, while U.S. domestic issuers are required to file their annual report on Form 10-K within 90 days after the end of each fiscal year. Foreign private issuers are also exempt from certain parts of the Regulation Fair Disclosure, aimed at preventing issuers from making selective disclosures of material information. As a result of the above, an investor may not have the same protections afforded to shareholders of companies that are not foreign private issuers.
| 38 |
As a foreign private issuer and as permitted by the listing requirements of Nasdaq, we rely on certain home country governance practices rather than the corporate governance requirements of Nasdaq.
As a foreign private issuer, in accordance with Nasdaq Listing Rule 5615(a)(3), we comply with home country governance requirements and certain exemptions thereunder rather than complying with all the corporate governance requirements of Nasdaq.
Scottish law does not require that a majority of our board of directors consist of independent directors or that our board committees consist of entirely independent directors. Our board of directors and board committees, therefore, may include fewer independent directors than would be required if we were subject to Nasdaq Listing Rule 5605(b)(1). In addition, we will not be subject to Nasdaq Listing Rule 5605(b)(2), which requires that independent directors must regularly have scheduled meetings at which only independent directors are present. Also, Scottish law does not require the board of directors to have a nominations committee, and we do not plan on having such a committee.
We also have an exemption from the Nasdaq listing rules so as to follow the quorum rules for shareholder meetings under Scottish law. We also have an exemption from the Nasdaq listing rules so as to not be required to obtain shareholder approval for certain issuance of securities and shareholder approval of share option plans under the Nasdaq Listing Rule 5635.
We may lose our foreign private issuer status, which would then require us to comply with the Exchange Act’s domestic reporting regime and cause us to incur significant legal, accounting and other expenses.
In order to maintain our current status as a foreign private issuer, a majority of our outstanding ordinary shares (including those represented by ADSs) must continue to be either directly or indirectly owned of record by non-residents of the United States. If a majority of our outstanding ordinary shares (including those represented by the ADSs) are instead held by U.S. residents, then in order to continue to maintain our foreign private issuer status, (i) a majority of our executive officers or directors must not be U.S. citizens or residents, (ii) more than 50% of our assets must not be located in the United States, and (iii) our business must be administered principally outside the United States. Currently, the majority of our executive officers and directors will be resident in the United Kingdom and not United States citizens or residents, less than 50% of our assets will be located in the United States, and our business will be administered principally in the United Kingdom.
Losing our status as a foreign private issuer would require us to comply with all of the periodic disclosure and current reporting requirements of the Exchange Act applicable to U.S. domestic issuers. We may also be required to make changes in our corporate governance practices in accordance with various SEC and Nasdaq rules. The regulatory and compliance costs to us under U.S. securities laws, if we are required to comply with the reporting requirements applicable to a U.S. domestic issuer, may be significantly higher than the cost we would incur as a foreign private issuer. As a result, we would expect that a loss of foreign private issuer status will increase our legal and financial compliance costs and will make some activities highly time consuming and costly. We also expect that if we will be required to comply with the rules and regulations applicable to U.S. domestic issuers, it will make it more difficult and expensive for us to obtain director and officer liability insurance; we may therefore be required to accept reduced coverage or incur substantially higher costs to obtain coverage. These rules and regulations could also make it more difficult for us to attract and retain qualified members of our board of directors.
We do not intend to list any of our securities on any public securities exchange in the United Kingdom. This may limit the information available to our security holders.
Our ordinary shares and public Warrants are not listed in the United Kingdom. As a result, we are not, and will not be, subject to the reporting and other requirements of companies listed on a securities exchange in the United Kingdom. Accordingly, there may be less publicly available information concerning our company than there would be if we were a public company listed in the United Kingdom, notwithstanding our reporting under the SEC rules.
| 39 |
An active and liquid market for the ADSs and/or public Warrants may fail to develop, which could harm the market price of the ADSs and/or Warrants, and an investor may not be able to resell their ADSs and/ or Warrants at or above the acquisition price.
An active public trading market for the ADSs and public Warrants on the United States securities markets may not develop or be sustained. In the absence of an active trading market for the ADSs and/or Warrants, investors may not be able to sell their ADSs and Warrants at or above the price they paid for their securities or at the time when they would like to sell.
The market price of the ADSs and public Warrants may be volatile and investors could lose all or part of their investment.
The price of the securities of publicly traded emerging pharmaceutical and drug discovery and development companies has been highly volatile and is likely to remain highly volatile in the future. As a result of this volatility, investors may not be able to sell their ADSs and Warrants at or above the purchase price or when they want to sell their securities. The market price of the ADSs and Warrants may fluctuate significantly due to a variety of factors, including the following:
| ● | positive or negative results of testing and clinical trials by us, strategic partners or competitors; | |
| ● | delays in entering into strategic relationships with respect to development or commercialization of our investigational GD-T cell therapy or any future therapeutic candidates; | |
| ● | entry into strategic relationships on terms that are not deemed to be favorable to us; | |
| ● | technological innovations or commercial therapeutic introductions by competitors; | |
| ● | changes in government regulations and healthcare payment systems; | |
| ● | developments concerning proprietary rights, including patent and litigation matters; | |
| ● | public concern relating to the commercial value or safety of any of our investigational GD-T cell therapy or any future therapeutic candidates; | |
| ● | negative publicity or public perception of the use of GD-T cells as a treatment therapy; | |
| ● | financing or other corporate transactions; | |
| ● | publication of research reports or comments by securities or industry analysts; | |
| ● | the trading volume of the ADSs and Warrants on Nasdaq; | |
| ● | sales of our ordinary shares, including through deposit of additional ordinary shares with the depositary for the ADSs, by us, members of our senior management and directors or our shareholders or the anticipation that such sales may occur in the future; | |
| ● | general market conditions in the pharmaceutical industry or in the economy as a whole; | |
| ● | general economic, political, and market conditions and overall market volatility in the United States or the UK as a result of the COVID-19 pandemic or other pandemics or similar events; and | |
| ● | other events and factors, many of which are beyond our control. |
These and other market and industry factors may cause the market price and demand for our securities to fluctuate substantially, regardless of our actual operating performance, which may limit or prevent investors from readily selling their ADSs and Warrants and may otherwise negatively affect the liquidity of the ADSs and Warrants. In addition, the stock market in general, and pharmaceutical companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies.
| 40 |
The public Warrants are speculative in nature.
The public Warrants merely represent the right to acquire our ordinary shares at a fixed cash price, for a limited period of time. If the Warrants are not exercised before they expire, in six years, the Warrants will never provide any value to the holder thereof. It is usual that the price of a warrant in the public market is more volatile than that of the corresponding shares for which it is exercisable. Therefore, investors should expect the price of a Warrant to be fluctuate to a greater degree than our ADSs, and correspondingly be more speculative.
Holders of our public Warrants will not have any rights of the holders of ordinary shares until such Warrants are exercised.
The public Warrants do not confer any of the rights afforded to the holders of our ordinary shares, even those ordinary shares held through ADSs, such as voting rights or the right to receive dividends, but rather merely represent the right to acquire ordinary shares at a fixed price.
We have a significant number of public Warrants outstanding, each Warrant to purchase one ADS, which may be exercised at a current cash exercise price of $4.25 per ADS. There is no assurance that they will be exercised and that they will provide funding for the Company.
As at March 1, 2022, there were approximately 15,798,620 public Warrants outstanding and there were an additional 7,944,486 warrants, options and other derivative securities outstanding, each of which currently is exercisable for one ordinary share. We also may be required to issue additional warrants in connection with the conversion of certain outstanding loan notes. For the public Warrants to be exercised on a cash basis, we must maintain an effective registration statement with the SEC at the time of their exercise. It is not expected that any of the derivative securities will be exercised for cash unless the price of an ADS in the market is substantially above the then exercise price. There can be no assurance that our ADS price will be sufficiently high on a sustained basis to encourage warrant holders to exercise their derivative securities, such as the public Warrants.
The public Warrants have a number of restrictions and reset provisions which may limit aspects of our operations and capital raising.
The public Warrant terms have restrictions on our ability to issue ordinary shares in a number of situations. For example, for the period during which the lock up agreements are in place, we have limits on our ability to issue ordinary shares under our incentive plans. Another restriction, one on our capital raising, is an exercise price reset provision; if we issue any ordinary shares, including instruments convertible into ordinary shares, at a per share price or conversion price less than the exercise price, the then the exercise price of the Warrants will be reduced to the lower issue price permanently. The Warrants have anti-dilution provisions including those for recapitalization transactions such as a reverse stock split, stock dividend and forward stock split, and protective provisions in the event of a rights offering, cash or asset dividend, and fundamental transactions consummated by the company where it is not the survivor. The Warrant has buy-in protection and cash penalties if we do not issue the securities underlying them on a timely basis. The six year term and number of Warrants in combination with the registration obligation will be an overhang on the market while the Warrants are outstanding. This overhang may limit our ability to raise capital when needed at a price that represents the value of the company. The Warrants do not have a redemption provision by which we can either encourage their exercise or terminate the Warrants.
The large number of public Warrants may aid an insurgent in seeking control of the company.
It is typical that a publicly traded warrant will trade at a price that is equal to the difference of the exercise price and the then market price of an ADS. This may result in our public Warrant trading at a low market price when compared to the price of an ADS in the market, thus making it possible to acquire a large number of the public Warrants for a low overall investment. The Warrants do not have any exercise limitation percentage. Thus, a potential insurgent may buy a large number of Warrants at a low overall purchase price and ultimately be able to control the company, directly or indirectly, through the Warrants, a substantial percentage of the company.
| 41 |
The ordinary shares that will become eligible for future sale may adversely affect the market for the ADSs and/or Warrants.
Subject to various lock up agreements to which our shareholders and holders of the Convertible Loan Notes have agreed, which have various leak out provisions, early termination provisions and exceptions, many of our shareholders are eligible to sell all or some of their ordinary shares by means of depositing them with the depositary in exchange for ADSs and then trading the ADSs through ordinary brokerage transactions, in the open market pursuant to Rule 144, promulgated under the Securities Act. Additionally, we have registered for resale ADSs and Warrants held by shareholders who converted outstanding Convertible Loan Notes into equity in connection with our February 2022 IPO or thereafter upon interest payment dates, which are subject to lock up agreements with leak out and early termination provisions. Any substantial sale of our ordinary shares, when represented by ADSs, and the public Warrants pursuant to Rule 144 or pursuant to any resale prospectus may have a material adverse effect on the public market price of the ADSs and public Warrants.
We incur increased costs as a result of operating as a Scottish public company listed in the U.S., and our board of directors is required to devote substantial time to compliance requirements and corporate governance practices.
As a Scottish public company listed in the U.S., we incur significant legal, accounting and other expenses that we did not incur as a private company. In addition, the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act, the listing requirements of Nasdaq, and other applicable securities rules and regulations impose various requirements on foreign reporting public companies, including the establishment and maintenance of effective disclosure and financial controls and corporate governance practices. Our board of directors, management and other personnel devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations increase our annual legal and financial compliance costs and make some activities more time-consuming and costly. For example, we expect that these rules and regulations may make it more difficult and more expensive for us to obtain director and officer liability insurance, which in turn could make it more difficult for us to attract and retain qualified members of our board of directors.
However, these rules and regulations are often subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. This could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices.
Pursuant to Section 404 of the Sarbanes-Oxley Act, or Section 404, we are required to furnish a report by our board of directors on our internal control over financial reporting, commencing with our second annual report. However, while we remain an emerging growth company, we are not required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To achieve compliance with Section 404 within the prescribed period, we will be engaged in a process to document and evaluate our internal controls over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, potentially engage outside consultants and adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. Despite our efforts, there is a risk that we will not be able to conclude, within the prescribed timeframe, that our internal controls over financial reporting are effective as required by Section 404. If we identify one or more material weaknesses, it could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements.
We are implementing appropriate accounting policies, processes and controls to comply with our expected expansion in scale of operations and with Section 404. These activities include identifying and recruiting additional individuals with requisite expertise to assist in implementation activities designed to strengthen our internal control over financial reporting to avoid control deficiencies and initiating the design and implementation of improvements to our financial control environment to address our future needs. However, we cannot give assurance that the measures we have taken to date, and actions we plan to take in the future, will be sufficient to prevent or avoid potential future material weaknesses in our controls.
| 42 |
If we are unsuccessful in building an appropriate accounting infrastructure, we may not be able to prepare and disclose, in a timely manner, our financial statements and other required disclosures, or comply with existing or new reporting requirements. Any failure to report our financial results on an accurate and timely basis could result in sanctions, lawsuits, delisting of our shares from Nasdaq or other adverse consequences that would materially harm our business. If we cannot provide reliable financial reports or prevent fraud, our business and results of operations could be harmed and investors could lose confidence in our reported financial information. Any of the foregoing occurrences, should they come to pass, could negatively impact the public perception of our company, which could have a negative impact on the price of our publicly traded securities or our ability to sell other securities.
We are an “emerging growth company” under the federal securities laws and we cannot be certain if the reduced disclosure requirements applicable to emerging growth companies will make our securities less attractive to investors.
We are an “emerging growth company,” as defined in Section 2(a) of the Securities Act, and we may take advantage of certain exemptions from various reporting requirements that are applicable to public companies that are not “emerging growth companies” including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation, and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and shareholder approval of any golden parachute payments not previously approved. We cannot predict if investors will find our securities less attractive because we may rely on these exemptions. Investors may be unable to compare our business with other companies in our industry if they believe that our reporting is not as transparent as other companies in our industry. If some investors, including persons considering an investment in the company, find our securities less attractive as a result, there may be a less active trading market for the our public securities, and the prices of these securities may be more volatile.
We will remain an “emerging growth company” for up to five years, although we will lose that status sooner if our revenues exceed $1 billion (or equivalent), if we issue more than $1 billion (or equivalent) in non-convertible debt in a three-year period, or if the market value of our ordinary shares that is held by non-affiliates exceeds $700 million (or equivalent) as of any June 30.
Holders of our ordinary shares will have their rights as a shareholder governed by Scottish law, and those rights differ from the rights of shareholders under U.S. law.
We are a public limited company under the laws of Scotland and United Kingdom. Therefore, the rights of holders of our ordinary shares, including those represented by ADSs, are governed by the corporate law of Scotland and the United Kingdom and by our memorandum of association and articles. The statutory framework that governs the Company is the Companies Act 2006 which is a UK-wide act and references to the “UK Law” are to UK-wide legislation. These rights differ from the typical rights of shareholders in U.S. corporations. In certain cases, facts that, under U.S. law, would entitle a shareholder in a U.S. corporation to claim damages may not give rise to a cause of action or claim for damages under Scottish law. For example, the rights of shareholders to bring proceedings against the Company or against our directors or officers in relation to public statements are more limited under Scottish law and UK Law than under the civil liability provisions of the U.S. securities laws.
Investors may face difficulties in protecting their interests, and their ability to protect their rights through the U.S. federal courts may be limited, because we are incorporated outside the United States, conduct most of our operations outside the United States, and most of our directors and senior management reside outside the United States.
We are incorporated and have our registered office in, and are currently existing under the laws of, Scotland. In addition, most of our tangible assets are located, and most of our senior management and certain of our directors reside, outside of the United States. As a result, it may not be possible to serve process within the United States on certain directors or us or to enforce judgments obtained in U.S. courts against such directors or us based on civil liability provisions of the securities laws of the United States.
| 43 |
The United States and the UK do not currently have a treaty providing for recognition and enforcement of judgments (other than arbitration awards) in civil and commercial matters. Consequently, a final judgment for payment of money given by a court in the United States, whether or not predicated solely upon U.S. securities laws, would not automatically be recognized or enforceable in the UK. In addition, uncertainty exists as to whether courts of Scotland would entertain original actions brought in Scotland against us or our directors or senior management predicated upon the securities laws of the U.S. or any state in the U.S. Any final and conclusive monetary judgment for a definite sum obtained against us in U.S. courts would be treated by the courts of Scotland as a cause of action in itself and sued upon as a debt at common law so that no retrial of the issues would be necessary, provided that certain requirements are met.
Whether these requirements are met in respect of a judgment based upon the civil liability provisions of the U.S. securities laws, including whether the award of monetary damages under such laws would constitute a penalty, is subject to determination by the court making such decision. If the courts of Scotland give a judgment for the sum payable under a U.S. judgment, the Scottish judgment will be enforceable by methods generally available for this purpose. These methods generally permit the courts of Scotland discretion to prescribe the manner of enforcement.
As a result, U.S. investors may not be able to enforce against us or certain of our directors any judgments obtained in U.S. courts in civil and commercial matters, including judgments under the U.S. federal securities laws.
As a Scottish public limited company, certain capital structure decisions will require shareholder approval, which may limit our flexibility to manage our capital structure.
Scottish law provides that a board of directors may only allot shares (or grant rights to subscribe for or to convert any security into shares) with the prior authorization of shareholders, such authorization stating the aggregate nominal amount of shares that it covers and being valid for a maximum period of five years, each as specified in the articles of association or relevant ordinary resolution passed by shareholders at a general meeting. Once allotted, the board of directors are free to issue the shares without further shareholder approval. The authority from our shareholders to allot additional shares for a period of five years from January 14, 2022 was included in the ordinary resolution passed by our shareholders on January 14, 2022, which authorization will need to be renewed upon expiration (i.e., at least every five years) but may be sought more frequently for additional five-year terms (or any shorter period).
Scottish law also generally provides shareholders with pre-emptive rights when new shares are issued for cash. However, it is possible for the articles of association, or for shareholders to pass a special resolution at a general meeting, being a resolution passed by the members (or of a class of members) of a company by a majority of not less than 75%, to disapply pre-emptive rights. Such a disapplication of pre-emptive rights may be for a maximum period of up to five years from the date of adoption of the articles of association, if the disapplication is contained in the articles of association, but not longer than the duration of the authority to allot shares to which this disapplication relates or from the date of the shareholder special resolution, if the disapplication is by shareholder special resolution. In either case, this disapplication would need to be renewed by our shareholders upon its expiration (i.e., at least every five years). Such authority from our shareholders to disapply pre-emptive rights for a period of five years was included in the special resolution passed by our shareholders on, January 14, 2022, which disapplication will need to be renewed upon expiration (i.e., at least every five years) to remain effective, but may be sought more frequently for additional five-year terms (or any shorter period).
Scottish law also generally prohibits a public company from repurchasing its own shares without the prior approval of shareholders by ordinary resolution, being a resolution passed by a simple majority of votes cast, and other formalities. Such approval may be for a maximum period of up to five years.
Our business and results of operations may be negatively impacted by the UK’s withdrawal from the EU.
The UK withdrew from the EU effective on January 31, 2020, and the transition period ended on December 31, 2020, which we refer to as Brexit. The future regulations that will apply in the UK following the transition period (including financial laws and regulations, tax and free trade agreements, intellectual property rights, data protection laws, supply chain logistics, environmental, health and safety laws and regulations medicine licensing and regulations, immigration laws and employment laws), have yet to be fully addressed and continue to be in transition, subject to change. The overall lack of clarity on future UK laws and regulations and their interaction with the EU laws and regulations may negatively impact foreign direct investment in the UK, increase costs, depress economic activity and restrict access to capital. As we are headquartered in the UK and have operations and clinical trials in the United Kingdom and EU, it is possible that Brexit may impact some or all of our current operations and otherwise how we conduct business. For example, Brexit may impact our ability to freely move employees from our headquarters in the UK to other locations in Europe, and it may impact the ability of European therapists to move freely to the UK in order to complete part of their training or work on our clinical trials there.
| 44 |
The long-term effects of Brexit will depend in part on the agreements the UK made during the Brexit transition period and thereafter to retain access to markets in the EU. The Brexit withdrawal from the EU is unprecedented, and it is unclear how the UK’s access to the European single market for goods, capital, services and labor within the EU, or single market, and the wider commercial, legal and regulatory environment, will impact our current and future operations (including business activities conducted by third parties and contract manufacturers on our behalf) and clinical activities in the UK In addition to the foregoing, our UK operations support our current and future operations and clinical activities in the EU and European Economic Area, or EEA, and these operations and clinical activities could be disrupted by Brexit.
We may also face new regulatory costs and challenges that could have an adverse effect on our operations as a result of Brexit. The UK could lose the benefits of global trade agreements negotiated by the EU on behalf of its member states, which may result in increased trade barriers that could make our doing business in the EU and the EEA more difficult. Since the regulatory framework in the UK covering quality, safety and efficacy of therapeutic substances, clinical trials, marketing authorization, commercial sales and distribution of therapeutic substances is derived from EU directives and regulations, Brexit could materially impact the future regulatory regime with respect to the approval of our GD-T cell therapy or any future therapeutic candidates in the UK. For instance, in November 2017, EU member states voted to move the EMA, the EU’s regulatory body, from London to Amsterdam. Operations in Amsterdam commenced in March 2019, and the move itself may cause significant disruption to the regulatory approval process in Europe. It remains to be seen how, if at all, Brexit will impact regulatory requirements for therapeutic candidates and therapies in the UK. Any delay in obtaining, or an inability to obtain, any regulatory approvals, as a result of Brexit or otherwise, would delay or prevent us from commercializing our investigational GD-T cell therapy or future therapeutic candidates in the UK and/or the EU and restrict our ability to generate revenue and achieve and sustain profitability. We may be forced to restrict or delay efforts to seek regulatory approval in the UK and/or EU for GD-T cell therapy or any future therapeutic candidates, which could significantly and materially harm our business.
We expect that Brexit, in the near and middle term will lead to certain legal uncertainties and potentially divergent national laws and regulations as the UK determines which EU laws to replicate or replace, including those related to data privacy and the regulation of medicinal products, as described above. Any of these effects of Brexit, and others we cannot anticipate, could negatively impact our business and results of operations.
Our business may be subject to risks related to possible Scottish independence from the UK
The possibility of Scottish independence from the UK creates a range of uncertainties for Scotland based business in general, which would require careful assessment by the board of directors and management as political events develop. There could be changes in currency, taxation, general legislation, regulations and trading arrangements and agreements, together with economic prospects more generally. It is not possible to predict the effect of Scottish independence if it were to occur and the changes introduced could have only limited effect on the business, be beneficial to the business or could have a material adverse effect on the business’ revenue, financial condition, profitability, prospects and results of operations.
A transfer of ordinary shares, other than one effected by means of the transfer of book-entry interests, such as through our ADS program, may be subject to United Kingdom stamp duty.
The transfer of our ordinary shares effected by means of the transfer of book entry interests through our ADS program will generally not be subject to United Kingdom stamp duty. However, if an investor holds its ordinary shares directly rather than beneficially through the ADS program, any transfer of ordinary shares (including into the ADS program with a view to trading) would be likely to be subject to United Kingdom stamp duty currently at the rate of 1.5% of the higher of the price paid or the market value of the shares acquired.
| 45 |
General Risk Factors
Exchange rate fluctuations may materially affect our results of operations and financial condition.
Due to the international scope of our operations, the financial reporting of our assets, earnings and cash flows are influenced by movements in exchange rates of several currencies, when comparing our results among different currencies such as the U.S. dollar, the pound sterling and the euro. Our reporting currency and our functional currency is the pound sterling and the majority of our operating expenses are paid in pound sterling. We regularly acquire services, consumables and materials in U.S. dollars, pound sterling and the euro. Further potential future revenue may be derived from non-United Kingdom jurisdictions, particularly from the United States. As a result, our business and the value of our ordinary shares, including those represented by the ADSs and underlying the Warrants, may be affected by fluctuations in foreign exchange rates between the pound sterling and these other currencies, which may have a significant impact on our results of operations and cash flows from period to period. Currently, we do not have any exchange rate hedging arrangements in place.
Collaborations, whether through joint ventures, licensing, development arrangements, and other forms of agreements, will be important to our overall business development.
In common with many development stage biotechnology companies an element of our business plan is consider entering into collaborative arrangements with larger pharmaceutical and biotechnology companies. We expect that future collaborations will provide us with important expertise, aid in product development, conducting drug trials, facilitate market entry and may provide some level of funding or future revenue. Notwithstanding our belief that collaborations will be beneficial to us, any collaboration arrangement may by their nature pose a number of risks, including the following:
| ● | collaborators have significant discretion in determining the efforts and resources that they will apply to a project; | |
| ● | collaborators may not perform their obligations as expected; | |
| ● | collaborators may dispute the amounts of payments owed; | |
| ● | collaborators may not pursue development and commercialization of any product candidates that achieve regulatory approval or may elect not to continue or renew development or commercialization programs or license arrangements |
In the past, we have entered into collaborative arrangements with two partners, bluebird bio, Inc. (USA) and Nipro Corporation (Japan), which involved funded or partly funded preclinical collaboration. Neither collaboration involve us in any current clinical or development activity or are generating any current cash receipts for us. It is uncertain if these collaborations will generate any future cash receipts or obligations for TCB.
As a company based outside of the United States, our business is subject to economic, political, regulatory and other risks associated with international operations.
Our business is based in the United Kingdom and is subject to risks associated with conducting business outside of the United States. Many of our suppliers and clinical trial relationships are located outside the United States, primarily in the United Kingdom and in the EU. Accordingly, our future results could be harmed by a variety of factors, including:
| ● | economic weakness, including inflation, or political change; | |
| ● | differing and changing regulatory requirements for product approvals; |
| 46 |
| ● | differing jurisdictions could present different issues for securing, maintaining or obtaining freedom to operate in such jurisdictions; | |
| ● | potentially reduced protection for intellectual property rights; | |
| ● | difficulties in compliance with different, complex and changing laws, regulations and court systems of multiple jurisdictions and compliance with a wide variety of foreign laws, treaties and regulations; | |
| ● | changes in non-U.S. currency exchange rates of the pound sterling, U.S. dollar, euro and currency controls; | |
| ● | changes in a specific country’s or region’s political or economic environment, including the implications of the recent action of the United Kingdom withdrawing from the European Union and efforts related to Scottish independence; | |
| ● | customs, tariffs and trade barriers, trade protection measures, import or export licensing requirements or other restrictive actions by governments; | |
| ● | differing medical product reimbursement regimes and price controls; | |
| ● | compliance with tax, employment, immigration and labor laws for employees living or traveling abroad, including, for example, the variable tax treatment in different jurisdictions of options granted under our share option schemes or equity incentive plans; | |
| ● | workforce uncertainty in countries where labor unrest is more common than in the United Kingdom and the United States; | |
| ● | difficulties associated with staffing and managing international operations, including differing labor relations; and | |
| ● | business interruptions resulting from geo-political actions, including war and terrorism, or natural disasters including earthquakes, typhoons, floods and fires. |
The conflict between Russia and Ukraine currently does not have any material impact on the company.
Our operations primarily are undertaken in the United Kingdom and the resources we use primarily are domestically available. We have not specifically sourced any resources for our operations from the Ukraine. We may be generally impacted by the macro-economic effects of international sanctions and the effects of inflation, as it would affect all businesses.
Computer system failures, cyber-attacks or deficiencies in our or related parties’ cyber security could result in a material disruption of our product development programs, compromise sensitive information related to our business or trigger contractual and legal obligations, any of which could potentially expose us to liability or reputational harm or otherwise adversely affect our business and financial results.
We have implemented our security measures designed to protect the information (including but not limited to intellectual property, proprietary business information and personal information) in our possession, custody or control. Our internal computer systems and those of current and future third parties (such as vendors, CROs, collaborators or others) on which we rely may fail and are vulnerable to breakdown, breach, interruption or damage from computer viruses, computer hackers, malicious code, employee error or malfeasance, theft or misuse, denial-of-service attacks, sophisticated nation-state and nation-state-supported actors, unauthorized access, natural disasters, terrorism, war, telecommunication and electrical failures or other compromise. Despite our security practices, there is a risk that we may be subject to phishing and other cyberattacks in the future. The risk of a security breach or disruption, particularly through cyber-attacks or cyber intrusion, including by computer hackers, foreign governments and cyber terrorists, has generally increased as the number, intensity and sophistication of attempted attacks and intrusions from around the world have increased. We may not be able to anticipate all types of security threats, and we may not be able to implement preventive measures effective against all such security threats. The techniques used by cyber criminals change frequently, may not be recognized until launched, and can originate from a wide variety of sources, including outside groups such as external service providers, organized crime affiliates, terrorist organizations or hostile foreign governments or agencies. Our information technology and other internal infrastructure systems, including corporate firewalls, servers, leased lines and connection to the Internet, face the risk of systemic failure that could disrupt our operations. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our development programs and our business operations. For example, the loss of clinical trial data from completed or future clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. Likewise, we rely on third parties for the manufacture of our product candidates or any future product candidates and to conduct clinical trials, and similar events relating to their computer systems could also have a material adverse effect on our business. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate use, disclosure of or access to confidential or proprietary information, we could incur liability, our competitive position could be harmed and the further development and commercialization of our product candidates or any future product candidates could be hindered or delayed. If we were to experience a significant cybersecurity breach of our information systems or data, the costs associated with the investigation, remediation and potential notification of the breach to counterparties, data subjects, regulators or others could be material. In addition, our remediation efforts may not be successful. Moreover, if the information technology systems of our vendors, CROs, collaborators or other contractors or consultants become subject to disruptions or security breaches, we may have insufficient recourse against such third parties and we may have to expend significant resources to mitigate the impact of such an event, and to develop and implement protections to prevent future events of this nature from occurring. If we do not allocate and effectively manage the resources necessary to build and sustain the proper technology and cybersecurity infrastructure, we could suffer significant business disruption, including transaction errors, supply chain or manufacturing interruptions, processing inefficiencies, data loss or the loss of or damage to intellectual property or other proprietary information. Furthermore, any such event that leads to unauthorized access, use, or disclosure of personal information, including personal information regarding clinical trial participants or employees, could harm our reputation, compel us to comply with federal and/or state breach notification laws and foreign law equivalents, cause us to breach our contractual obligations, subject us to mandatory corrective action, and otherwise subject us to liability under laws, regulations and contracts that protect the privacy and security of personal information, which could result in significant legal and financial exposure and reputational damages. As cyber threats continue to evolve, we may be required to incur significant additional expenses in order to enhance our protective measures or to remediate any information security vulnerability.
In addition, in response to the ongoing COVID-19 pandemic, varying parts of our workforce are currently working remotely on a part- or full-time basis. This could increase our cyber security risk, create data accessibility concerns, and make us more susceptible to communication disruptions. Any of the foregoing could have a material adverse effect on our business, financial condition, results of operations or prospects.
If we are not able to maintain and enhance our reputation and brand recognition, our business, financial condition and results of operations will be harmed.
We believe that maintaining and enhancing our reputation and brand recognition is critical to our relationships with existing and future third-party therapy locations, therapists, patients and collaborators, and to our ability to attract clinics to become our third-party therapy locations offering our therapies. The promotion of our brand may require us to make substantial investments, and we anticipate that, as our market becomes increasingly competitive, these marketing initiatives may become increasingly difficult and expensive. Brand promotion and marketing activities may not be successful or yield increased revenue, and to the extent that these activities yield increased revenue, the increased revenue may not offset the expenses we incur and our business, financial condition and results of operations could be harmed. In addition, any factor that diminishes our reputation or that of our management, including failing to meet the expectations of our network of third-party therapy locations, therapists and patients, could harm our reputation and brand and make it substantially more difficult for us to attract new third-party therapy locations, therapists and patients. If we do not successfully maintain and enhance our reputation and brand recognition, our business may not grow and we could lose our relationships with third-party therapy sites, therapists and patients, which would harm our business, financial condition and results of operations.
| 47 |
We are subject to anti-corruption laws, export control laws, customs laws, sanctions laws and other laws governing our operations. If we fail to comply with these laws, we could be subject to civil or criminal penalties, other remedial measures and legal expenses, be precluded from manufacturing our products and developing and selling our investigational therapies or any future therapeutic candidates or be required to develop and implement costly compliance programs, which could adversely affect our business, results of operations and financial condition.
Our operations are subject to anti-corruption laws, including the UK Bribery Act 2010, or Bribery Act, the U.S. Foreign Corrupt Practices Act of 1977, as amended, or FCPA, and other anti-corruption laws that apply in countries where we do business and may do business in the future. The Bribery Act, FCPA and these other laws generally prohibit us, our officers, and our employees and intermediaries from bribing, being bribed or making other prohibited payments to government officials or other persons to obtain or retain business or gain some other business advantage.
The Bribery Act, the FCPA and these other laws generally prohibit us and our employees and intermediaries from authorizing, promising, offering, or providing, directly or indirectly, a financial or other advantage to government officials or other persons to induce them to improperly perform a relevant function or activity (or reward them for such behavior).
Under the Bribery Act, we may also be liable for failing to prevent a person associated with us from committing a bribery offense. We, along with those acting on our behalf and our commercial partners, operate in a number of jurisdictions that pose a high risk of potential Bribery Act or FCPA violations, and we participate in collaborations and relationships with third parties whose corrupt or illegal activities could potentially subject us to liability under the Bribery Act, FCPA or local anti-corruption laws, even if we do not explicitly authorize or have actual knowledge of such activities. In addition, we cannot predict the nature, scope or effect of future regulatory requirements to which our international operations might be subject or the manner in which existing laws might be administered or interpreted.
Compliance with the FCPA, in particular, is expensive and difficult, particularly in countries in which corruption is a recognized problem. In addition, the FCPA presents particular challenges in the pharmaceutical industry, because, in many countries, hospitals are operated by the government, and doctors and other hospital employees are considered foreign officials. Certain payments to hospitals in connection with clinical trials and other work have been deemed to be improper payments to government officials and have led to FCPA enforcement actions. Need to dedicate additional resources to comply with numerous laws and regulations in each jurisdiction in which we plan to operate.
We may in the future operate in jurisdictions that pose a high risk of potential Bribery Act or FCPA violations, and we may participate in collaborations and relationships with third parties whose actions could potentially subject us to liability under the Bribery Act, FCPA or local anti-corruption laws. In addition, we cannot predict the nature, scope or effect of future regulatory requirements to which our international operations might be subject or the manner in which existing laws might be administered or interpreted. If we expand our operations, we will need to dedicate additional resources to comply with numerous laws and regulations in each jurisdiction in which we plan to operate.
We are also subject to other laws and regulations governing our international operations, including regulations administered by the governments of the UK and the U.S., and authorities in the EU, including applicable export control regulations, economic sanctions on countries and persons, customs requirements and currency exchange regulations, collectively referred to as the Trade Control laws. In addition, various laws, regulations and executive orders also restrict the use and dissemination outside of the United States, or the sharing with certain non-U.S. nationals, of information classified for national security purposes, as well as certain products and technical data relating to those products. If we expand our presence outside of the U.S., it will require us to dedicate additional resources to comply with these laws, and these laws may preclude us from manufacturing our products and developing and selling our investigational therapies or any future therapeutic candidates outside of the United States, which could limit our growth potential and increase our development costs.
There is no assurance that we will be completely effective in ensuring our compliance with all applicable anti-corruption laws, including the Bribery Act, the FCPA or other legal requirements, including Trade Control laws. If we are not in compliance with the Bribery Act, the FCPA and other anti-corruption laws or Trade Control laws, we may be subject to criminal and civil penalties, disgorgement and other sanctions and remedial measures, and legal expenses, which could have an adverse impact on our business, financial condition, results of operations and liquidity. Any investigation of any potential violations of the Bribery Act, the FCPA, other anti-corruption laws or Trade Control laws by UK, U.S. or other authorities could also have an adverse impact on our reputation, our business, results of operations and financial condition.
| 48 |
Because we are subject to environmental, health and safety laws and regulations, we may become exposed to liability and substantial expenses in connection with environmental compliance or remediation activities which may adversely affect our business and financial condition.
Our operations, including our research, development, testing and manufacturing activities, are subject to numerous environmental, health and safety laws and regulations. These laws and regulations govern, among other things, the controlled use, manufacture, handling, release and disposal of and the maintenance of a registry for, hazardous materials, such as chemical solvents, human cells, carcinogenic compounds, mutagenic compounds and compounds that have a toxic effect on reproduction, laboratory procedures and exposure to blood-borne pathogens
We may incur significant costs to comply with these current or future environmental and health and safety laws and regulations. Furthermore, if we fail to comply with such laws and regulations, we could be subject to fines or other sanctions.
As with other companies engaged in activities similar to ours, we face a risk of environmental liability inherent in our current and historical activities, including liability relating to releases of or exposure to hazardous materials and, as a result, may incur material liability as a result of such release or exposure. Environmental, health and safety laws and regulations are becoming more stringent. We may incur substantial expenses in connection with any current or future environmental compliance or remediation activities, in which case, our production and development efforts may be interrupted or delayed and our financial condition and results of operations may be materially adversely affected. In the event of an accident involving such hazardous materials, an injured party may seek to hold us liable for damages that result.
Our internal computer systems, or those of our future collaborators or other contractors or consultants, may fail or suffer security breaches, which could result in a significant disruption of our product development programs and our ability to operate our business effectively.
Our internal computer systems and those of our current and any future collaborators and other contractors or consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. While we have not experienced any significant system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a disruption of our development programs and our business operations, whether due to a loss of our trade secrets or other proprietary information or other similar disruptions. For example, the loss of clinical trial data from completed or future clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability, our competitive position could be harmed and the further development and commercialization of our product candidates could be delayed.
We do not intend to pay dividends on our ordinary shares, including those represented by ADSs, so any returns will be limited to the market value of the ADSs.
We currently anticipate that we will retain future earnings for the development, operation, and expansion of our business and do not anticipate declaring or paying any cash dividends for the foreseeable future. In addition, we may enter into agreements that prohibit us from paying cash dividends without prior written consent from our contracting parties, or which include other terms prohibiting or limiting the amount of dividends that may be declared or paid on our ordinary shares, including those represented by the ADSs. Furthermore, under UK corporate law, a company’s accumulated realized profits, so far as not previously utilized by distribution or capitalization, must exceed its accumulated realized losses so far as not previously written off in a reduction or reorganization of capital duly made (on a non-consolidated basis), before dividends can be paid. In the future, were our dividend policy to change, a dividend or distribution may still be restricted from being declared and paid. For these reasons, any return to shareholders may therefore be limited to the appreciation of their shares, which may never occur.
| 49 |
Investors in our ADSs may not receive distributions on our ordinary shares or any other value applicable to them if it is illegal or impractical to make them available to holders of ADSs.
The depositary for the ADSs has agreed to pay to the ADS holders the cash dividends or other distributions it or the custodian receives on our ordinary shares or other deposited securities after deducting its fees and expenses. ADS holders will receive these distributions in proportion to the number of our ordinary shares that the ADSs represent. In accordance with the limitations set forth in the deposit agreement, however, it may be unlawful or impractical to make a distribution available to holders of ADSs. We have no obligation to take any other action to permit distribution on the ADSs, ordinary shares, rights or anything else to holders of the ADSs. This means that ADS holders may not receive the distributions we make on our ordinary shares or any value from them if it is unlawful or impractical to make them available to the ADS holder. These restrictions may have an adverse effect on the value of the ADSs.
Holders of the ADSs will not have the same voting rights as the holders of our ordinary shares, and may not receive voting materials or any other documents that would need to be provided to our shareholders pursuant in time to be able to exercise their right to vote.
Holders of the ADSs will not be able to exercise voting rights attaching to the ordinary shares represented by the ADSs. The deposit agreement provides that, upon receipt of notice of any meeting of holders of our ordinary shares, the depositary will fix a record date for the determination of ADS holders who shall be entitled to give instructions for the exercise of voting rights. Upon our request, the depositary shall distribute to the holders as of the record date: (i) the notice of the meeting or solicitation of consent or proxy sent by us; and (ii) a statement as to the manner in which instructions may be given by the holders. We cannot guarantee that ADS holders will receive the voting materials in time to ensure that they can instruct the depositary to vote the ordinary shares underlying their ADSs.
ADS holders will not be able to exercise their right to vote directly as a holder of ordinary shares, unless they surrender the ADSs they hold to the depositary and withdraw the ordinary shares underlying such ADSs. Holders of ADSs may not know about the meeting far enough in advance to cancel the ADSs and withdraw those ordinary shares. In addition, the depositary and its agents are not responsible for failing to carry out voting instructions or for the manner of carrying out voting instructions. As a result, holders of ADSs may not be able to exercise their right to vote, and there may be nothing they can do if the ordinary shares underlying their ADSs are not voted as they requested or if their shares cannot be voted.
Holders of ADSs may not be able to participate in equity offerings we may conduct from time to time.
Certain shareholders and holders of ADSs, including those in the United States, may, even in the case where preferential subscription rights have not been cancelled or limited, not be entitled to exercise such rights, unless the offering is registered or the ordinary shares are qualified for sale under the relevant regulatory framework. As a result, there is the risk that investors in ADSs may suffer dilution of their holdings should they not be permitted to participate in preference right equity or other offerings that we may conduct in the future.
Holders of ADSs may be subject to limitations on the transfer of their ADSs and the withdrawal of the underlying ordinary shares.
ADSs are transferable on the books of the depositary. However, the depositary may close its books at any time or from time to time when it deems expedient in connection with the performance of its duties. The depositary may refuse to deliver, transfer or register transfers of ADSs generally when our books or the books of the depositary are closed, or at any time if we or the depositary think it is advisable to do so because of any requirement of law, government or governmental body, or under any provision of the deposit agreement, or for any other reason, subject to the right of ADS holders to cancel their ADSs and withdraw the underlying ordinary shares. Temporary delays in the cancellation of the ADSs and withdrawal of the underlying ordinary shares may arise because the depositary has closed its transfer books or we have closed our transfer books, the transfer of ordinary shares is blocked to permit voting at a shareholders meeting or we are paying a dividend on our ordinary shares. In addition, ADS holders may not be able to cancel their ADSs and withdraw the underlying ordinary shares when they owe money for fees, taxes and similar charges and when it is necessary to prohibit withdrawals in order to comply with any laws or governmental regulations that apply to ADSs or to the withdrawal of ordinary shares or other deposited securities.
| 50 |
Holders of ADSs may not be entitled to a jury trial with respect to claims arising under the deposit agreement, which could result in less favorable outcomes to the plaintiff(s) in any such action.
The deposit agreement governing the ADSs representing our ordinary shares provides that, to the fullest extent permitted by law, owners and holders of ADSs irrevocably waive the right to a jury trial of any claim they may have against us or the depositary arising out of or relating to the ADSs or the deposit agreement.
If this jury trial waiver provision is not permitted by applicable law, an action could proceed under the terms of the deposit agreement with a jury trial. If we or the depositary oppose a jury trial demand based on the waiver, the court would determine whether the waiver was enforceable based on the facts and circumstances of that case in accordance with the applicable state and federal law. To our knowledge, the enforceability of a contractual pre-dispute jury trial waiver in connection with claims arising under the federal securities laws has not been finally adjudicated by the United States Supreme Court. However, we believe that a contractual pre-dispute jury trial waiver provision is generally enforceable, including under the law of the State of New York, which governs the deposit agreement, by a federal or state court in the City and County of New York, which has non-exclusive jurisdiction over matters arising under the deposit agreement. In determining whether to enforce a contractual pre-dispute jury trial waiver provision, courts will generally consider whether a party knowingly, intelligently and voluntarily waived the right to a jury trial. We believe that this is the case with respect to the deposit agreement and the ADSs. It is advisable that investors consult legal counsel regarding the jury waiver provision before entering into the deposit agreement.
If holders or beneficial owners of ADSs bring a claim against us or the depositary in connection with matters arising under the deposit agreement or the ADSs, including claims under federal securities laws, such holder or beneficial owner may not be entitled to a jury trial with respect to such claims, which may have the effect of limiting and discouraging lawsuits against us and/or the depositary. If a lawsuit is brought against us and/or the depositary under the deposit agreement, it may be heard only by a judge or justice of the applicable trial court, which would be conducted according to different civil procedures and may result in different outcomes than a trial by jury would have had, including results that could be less favorable to the plaintiff(s) in any such action, depending on, among other things, the nature of the claims, the judge or justice hearing such claims, and the venue of the hearing.
No condition, stipulation or provision of the deposit agreement or ADSs serves as a waiver by any holder or beneficial owner of ADSs or by us or the depositary of compliance with U.S. federal securities laws and the rules and regulations promulgated thereunder.
Holders of ADSs have limited choice of forum, which could limit their ability to obtain a favorable judicial forum for complaints against us, the depositary or our respective directors, officers or employees.
The deposit agreement governing the ADSs provides that: (i) the deposit agreement and the ADSs will be interpreted in accordance with the law of the State of New York; and (ii) as an owner of ADSs, the investor irrevocably agrees that any legal action arising out of the deposit agreement and the ADSs involving us or the depositary may only be instituted in a state or federal court sitting in the City and County of New York. Any person or entity purchasing or otherwise acquiring any the ADSs, whether by transfer, sale, operation of law or otherwise, shall be deemed to have notice of and have irrevocably agreed and consented to these provisions. This choice of forum provision may increase costs and limit the ability to bring a claim in a judicial forum that the ADS holder finds favorable for disputes with us, the depositary or our and the depositary’s respective directors, officers or employees, which may discourage such lawsuits against us, the depositary and our and the depositary’s respective directors, officers or employees. However, it is possible that a court could find such choice of forum provisions to be inapplicable or unenforceable. The enforceability of similar choice of forum provisions has been challenged in legal proceedings. It is possible that a court could find this type of provisions to be inapplicable or unenforceable.
To the extent that any such claims may be based upon federal law claims, Section 27 of the Exchange Act creates exclusive federal jurisdiction over all suits brought to enforce any duty or liability created by the Exchange Act or the rules and regulations thereunder. Furthermore, Section 22 of the Securities Act creates concurrent jurisdiction for federal and state courts over all suits brought to enforce any duty or liability created by the Securities Act or the rules and regulations thereunder. Accordingly, actions by our ADS holders to enforce any duty or liability created by the Exchange Act, the Securities Act or the respective rules and regulations thereunder must be brought in a federal court. Our ADS holders will not be deemed to have waived our compliance with the federal securities laws and the regulations promulgated thereunder.
| 51 |
If we are a “passive foreign investment company,” or a PFIC, in any particular year, a U.S. shareholder may be subject to adverse U.S. federal income tax consequences.
Under the Internal Revenue Code of 1986, as amended, or the Code, we will be a PFIC for any taxable year in which, after the application of certain look-through rules with respect to our subsidiaries, either (i) 75% or more of our gross income consists of passive income or (ii) 50% or more of the average quarterly value of our assets consists of assets that produce, or are held for the production of, passive income (including cash). Passive income includes, among other things, dividends, interest, certain non-active rents and royalties, and capital gains. Based on our operations, income, assets and certain estimates and projections, including as to the relative values of our assets and the treatment of amounts in respect of refundable tax credits from governmental entities we received, or are or may become entitled to receive, as gross income that is not passive income, we do not believe that we were a PFIC in 2020 and do not expect to be a PFIC for our 2021 taxable year. However, the determination whether we are a PFIC is a fact-intensive determination that must be made on an annual basis applying principles and methodologies that are in some circumstances unclear, and whether we will be a PFIC in 2022 or any future taxable year is uncertain because, among other things, (i) we currently own a substantial amount of passive assets, including cash, (ii) the valuation of our assets that generate non-passive income for PFIC purposes, including our intangible assets, is uncertain and may depend in part of the market price of the ADSs or, if applicable, our ordinary shares from time to time, which may fluctuate substantially, (iii) the treatment of amounts in respect of refundable tax credits from governmental entities we received, or are or may become entitled to receive, as gross income that is not passive income is uncertain, and (iv) the composition of our income may vary substantially over time. Accordingly, there can be no assurance that we will not be a PFIC for any taxable year, and our U.S. counsel expresses no opinion with respect to our PFIC status, or with respect to our expectations regarding our PFIC status in 2022 or any future taxable year.
If we are a PFIC for any taxable year during which a U.S. investor holds ADSs or ordinary shares, we would continue to be treated as a PFIC with respect to that U.S. investor for all succeeding years during which the U.S. investor holds the ADSs or ordinary shares, even if we ceased to meet the threshold requirements for PFIC status, unless certain exceptions apply. Such a U.S. investor may be subject to adverse U.S. federal income tax consequences, including (i) the treatment of all or a portion of any gain on the disposition of the ADSs or ordinary shares as ordinary income (and therefore ineligible for the preferential rates that apply to capital gains with respect to some U.S. investors), (ii) the application of a deferred interest charge on such gain and the receipt of certain dividends on the ADSs or the ordinary shares and (iii) compliance with certain reporting requirements. We do not intend to provide the information that would enable investors to make a qualified electing fund election, or a QEF Election, with respect to their holding of ADSs or ordinary shares that could mitigate the adverse U.S. federal income tax consequences to a U.S. investor should we be classified as a PFIC.
If we are a controlled foreign corporation for U.S. federal income tax purposes, there could be adverse U.S. federal income tax consequences to certain U.S. holders who own, directly, indirectly or by attribution, ten percent or more of our ordinary shares.
Each “Ten Percent Shareholder” (as defined below) in a non-U.S. corporation that is classified as a “controlled foreign corporation,” or a CFC, for U.S. federal income tax purposes generally is required to include in income for U.S. federal tax purposes such Ten Percent Shareholder’s pro rata share of the CFC’s “Subpart F income”, investment of earnings in U.S. property, and “global intangible low-taxed income”, even if the CFC has made no distributions to its shareholders. In addition, a Ten Percent Shareholder that realizes gain from the sale or exchange of shares in a CFC may be required to classify a portion of such gain as dividend income rather than capital gain. A non-U.S. corporation generally will be classified as a CFC for U.S. federal income tax purposes if Ten Percent Shareholders own, directly, indirectly or constructively (through attribution), more than 50% of either the total combined voting power of all classes of stock of such corporation entitled to vote or of the total value of the stock of such corporation.
A “Ten Percent Shareholder” is a United States person (as defined by the Code) who owns or is considered to own 10% or more of the total combined voting power of all classes of stock entitled to vote of such corporation or 10% or more of the total value of the stock of such corporation. The determination of CFC status is complex and includes attribution rules, the application of which is not entirely certain. A failure by a United States shareholder of a CFC to comply with its reporting obligations may subject the United States shareholder to significant monetary penalties and other adverse tax consequences, and may extend the statute of limitations. We cannot provide any assurances that we will assist U.S. holders in determining whether we or any of our non- U.S. subsidiaries are CFCs or whether any holder is a Ten Percent Shareholder. We also cannot guarantee that we will furnish information that may be necessary to comply with the aforementioned obligations. U.S. holders should consult their own advisors regarding the potential application of these rules.
| 52 |
| Item 4. | Information on the Company |
| A. | History and Development of the Company |
We are a public company with limited liability incorporated on October 25, 2021, pursuant to the laws of Scotland, under the name TC BioPharm (Holdings) plc. We were incorporated with nominal share capital for the purpose of becoming the ultimate holding company of TC BioPharm Limited, the company in which our principal operations are undertaken, and for the purpose of consummating the corporate reorganization described herein. TC BioPharm (Holdings) plc will not conduct any operations except those as the listed entity, as explained below.
TC BioPharm Limited was incorporated on July 1, 2013, as a private company with limited liability pursuant to the laws of Scotland and has conducted and will continue to conduct our principal operations. TC BioPharm Limited has two wholly owned subsidiaries:
| ● | TC BioPharm BV, The Netherlands – incorporated March 2019 | |
| ● | TC BioPharm (North America) Inc. – incorporated June 2021 |
These two subsidiaries have had limited operating activity since their incorporation. It is anticipated that TC BioPharm (North America) Inc. will develop operations and a management presence in the United States, with a view to expanding our product offerings into that jurisdiction in the future.
The corporate reorganization took place in several steps as follows:
| ● | On December 17, 2021, all shareholders in TC BioPharm Limited and holders of convertible loan notes in TC BioPharm Limited exchanged their shares and convertible loan notes for the same number and classes of newly issued shares and/or convertible loan notes in TC BioPharm (Holdings) Limited and, as a result, TC BioPharm Limited became a wholly owned subsidiary of TC BioPharm (Holdings) Limited. | |
| ● | On December 17, 2021, TC BioPharm (Holdings) Limited carried out a 10 for 1 forward split of all classes of its share capital. | |
| ● | On December 30, 2021, holders of various options to subscribe for shares in TC BioPharm Limited exchanged their options for equivalent options in TC BioPharm (Holdings) Limited. | |
| ● | On January 10, 2022, TC BioPharm (Holdings) Limited re-registered under the laws of Scotland as a public limited company, with a change of name to TC BioPharm (Holdings) plc. | |
| ● | Immediately prior to the completion of the initial public offering, the different classes and nominal values of issued share capital of TC BioPharm (Holdings) plc were reorganized into a single class of ordinary shares with the same nominal value. The ADSs represent a portion of these ordinary shares. |
| ● | On February 10, 2022, TC BioPharm (Holdings) plc completed an initial public offering on the Nasdaq Capital Market. Our ADSs and warrants are traded under the symbols TCBP and TCBP respectively. Our ordinary shares are not listed. Our registered office in the United Kingdom is located at Maxim 1, 2 Parklands Way, Holytown, Motherwell, ML1 4WR, Scotland, United Kingdom, and the telephone of our registered office is +44 (0) 141 433 7557. |
Our agent for service of process in the United States is TC BioPharm (North America) Inc., c/o Business Filings, Inc., 108 West 13th Street, Wilmington, Delaware 19801 and the telephone number is (800) 981-7183.
Our capital expenditures for the years ended December 31, 2019, 2020 and 2021 amounted to £2.0 million, £Nil million and £Nil million, respectively. These capital expenditures primarily consisted of property, plant and equipment, computer equipment and office equipment in the United Kingdom.
The SEC maintains an Internet site that contains reports, proxy information statements and other information regarding issuers that file electronically with the SEC. The address of that site is http://www.sec.gov. Our website address is www.tcbiopharm.com. Information contained in, or that can be accessed through, our website is not a part of, and shall not be incorporated by reference into, this document. We have included our website address in this document solely as an inactive textual reference.
| B. | Business |
Overview
TC BioPharm is a clinical-stage biopharmaceutical company focused on developing novel immunotherapy products based on our proprietary allogeneic gamma delta T (GD-T) cell platform. Harnessing the innate ability of GD-Ts has enabled TCB to develop a range of clinical-stage cell therapies designed to combat cancer and viral infection.
| 53 |
In-house clinical studies have demonstrated that TCB’s unmodified allogeneic GD-T products are (i) well tolerated and (ii) show preliminary evidence of disease modification in patients with the late-stage blood cancer, known as acute myeloid leukemia – AML. Based on clinical data generated by TCB, we believe that unmodified GD-Ts have the potential to treat all blood cancers.
TCB now is embarking on phase 2b-into-pivotal (phase 3) clinical studies with a view to launching its first oncology product for the treatment of AML during 2023. Clinical results generated thus far have enabled TCB to obtain FDA orphan drug status for treatment of AML.
In addition to unmodified allogenic GD-Ts for treatment of blood cancers, TCB also is developing an innovative range of genetically-modified CAR-T products for treatment of solid cancers. We believe that solid cancers are more difficult to treat than blood cancers and may require the addition of a CAR “chimeric antigen receptor” (i) to help therapeutic cells to “navigate” into diseased cancerous tissue and (ii) to retain therapeutic cells in-situ at the lesion for maximal efficacy (increased persistence).
In order to manufacture our portfolio of allogeneic products, we select the highest quality GD-T cells from healthy donors, activate the cells and grow them in large numbers at our in-house GMP-compliant manufacturing facility before administration to a patient in order to target and then destroy malignant or virally-infected tissues. We believe that TCB has introduced a step-change to our manufacturing platform by implementing a freeze-thaw process that will allow product to be shipped from cleanroom to patient without any shelf-life issue. Resulting products, we believe, will be more cost-effective and straightforward to ship form cleanroom to clinic.
Business Strategy
TC BioPharm has taken a step-wise approach to clinical development and commercialization. To achieve this, we have made the clinical transition from autologous GD-Ts to allogeneic GD-Ts to CAR-modified allogeneic GD-Ts. Our commercialization strategy is to introduce products firstly in blood cancers (AML initially) and then solid tumor indications.
Our strategic objective is to build a global therapeutic business with an extensive portfolio of GD-T cell-based products with the potential to significantly improve the outcomes of patients with cancer and infectious disease. In order to achieve our objective, TCB is focused on delivering success in the following areas:
Progress unmodified GD-T2s into Phase 2/3 clinical trials for the treatment of blood cancers
Having generated meaningful clinical data showing our product is well-tolerated in late-stage AML patients with no remaining treatment options, TCB aims to commence phase 2b-into pivotal (phase 3) clinical studies under the trial name ‘ACHIEVE’, with OmnImmune® during 2022 in AML patients who have failed to respond adequately to induction therapy. The aim is to provide a form of salvage therapy which will either stabilize the patient, thereby preventing disease progression, or delay the requirement for human stem cell transplant. Our initial trial centers will be in the UK and we anticipate treating our first patients in Q2 2022. Working on the premise that other blood cancers should respond to GD-Ts in a similar manner to AML, TCB plans to conduct clinical studies for OmnImmune® in other hematological malignancies in future.
OmnImmune® clinical program
Our OmnImmune® clinical program is an example of our stepwise approach to clinical development. The initial phase 1b/2a trials were undertaken using fresh cell-based product under the program number TCB002. For ease of reference, when discussing that specific trial, we refer the program as OmnImmune® (TCB002). The subsequent planned phase 2b-into pivotal (phase 3) clinical studies will use a frozen cell-based product under the program number TCB008-001. When discussing that specific trial, we refer the program as OmnImmune® (TCB008-001).
| 54 |
Unmodified GD-T2s for use in the treatment of infectious disease
Gamma-delta T cells are dysfunctional in patients with many severe viral diseases and TCB anticipates that its unmodified gamma delta T cell therapy platform will be used in due course to treat viral infections as well as cancers under the name ImmuniStim®. For example, during 2022 TCB developed a clinical trial protocol to treat patients with COVID 19. Because of the progress of the disease and absence of appropriate trial patients this trial is not currently being progressed, although we expect to continue our infectious disease program in future.
Progress CAR-modified GD-Ts into Phase 1 clinical trials for treatment of solid tumors
TCB aims to treat solid cancers using its patented co-stimulatory GD-T and is currently undergoing pre-clinical work to determine the most appropriate CAR construct and target indication.
Grow our business operations to support the increasing number of clinical-phase products in development
We believe that our existing cell and gene manufacturing facility in the UK has the capacity to support our committed clinical development plans. We plan to continue to build upon this to support expansion of our product pipelines to new assets and to grow our clinical team. We also will work closely with vendors to embrace emerging technologies in our manufacturing operations that are appropriate and optimized for our products to continually improve the quality and efficiency of our manufacturing systems. We believe that maintaining in-house control of these activities is critical to effective and efficient progression and we will continue to seek to build integrated business functions where possible.
Apply our discovery engine to target further diseases and add additional functionality to our products
As a platform technology, our co-stimulatory CAR-T GD-T cell system has a wealth of potential options to build added functionality into our cell-based platform. We plan to continue to innovate and partner in the field to augment our drug products and introduce next generation attributes. We also plan to continue to innovate our manufacturing and supply chains to efficiently scale our processes and simplify the interface with patients and healthcare professionals, whilst continually seeking to reduce manufacturing costs to improve patient access.
Expand our intellectual property portfolio and acquire additional technologies to augment our strong IP position
We intend to continue building on our technology platform, comprised of intellectual property, proprietary methods and know-how in the field of GD-T cells. These assets form the foundation for our ability, not only to strengthen our product pipeline, but also to successfully defend and expand our position as a leader in the field of GD-T based immune-oncology.
Our Pipeline
What are gamma delta T cells?
The immune system plays an important role in targeting and destroying cancer cells. One component has evolved to scan the body for diseased cells and eradicate them. In humans, GD-Ts arise as a number of different subtypes, defined by the sequence of the gamma and delta chains of the T-cell receptor (TCR) on the cell surface. The gammadelta2 (GD-T2) subtype typically is the most abundant of these cells in healthy humans, and its TCR- of anti-cancer immunity is GD-T cells – a type of white blood cell that express a variety of innate receptors, which mediated signaling has been fully characterized by researchers.
Virally-infected or cancerous cells become stressed and accumulate cell surface phosphoantigens (isopentenyl pyrophosphate – IPP’s) which are recognized by GD-T2 cells. Our proprietary technology platform includes the manufacturing of unmodified and genetically modified (CAR-T) GD-T cells as therapeutic candidates for use in clinical trials and commercialization. Almost all aspects of the value-chain from product manufacture, quality systems, clinical and regulatory are operated in-house by TC BioPharm. We believe this is one of our core competitive advantages, which we believe will contribute materially to our ability to overcome the challenging nature of developing new products.
| 55 |
Human lymphocytes comprise two groups of cells, B cells that generate antibodies for humoral immunity, and T cells that are responsible for cellular immune responses. In healthy individuals, GD-T cells generally represent between 1% and 10% of peripheral blood T lymphocytes and present one of the first lines of defense against a wide range of bacterial and viral pathogens, as well as surveillance for cancerous cells. GD-T cells have the ability to regulate the initial immune response in several ways, including recruitment of other immune cells such as neutrophils, dendritic cells and macrophages through production of various chemokines (Kirby et al., 2007). Depletion of GD-T cells leads to impaired host defense to lung infections, for example (Moore et al., 2000; Lockhart et al., 2006). The predominant subset of GD-T cells in the blood is the GD-T2, which mediates a variety of immune responses by direct cytolysis of cancer cells and infected cells, development of memory phenotypes and modulation of other immune cells. The gammadelta1 (GD-T1) is a functionally distinct subset of GD-T cells, which are a predominantly tissue resident population. GD-T1s are less well characterized, but their cytotoxic function also has been described in different liquid and solid tumors (Siegers & Lamb, 2014).
Both subsets of GD-T cells are thought to play a role in autoimmune disorders such as celiac disease, rheumatoid arthritis, autoimmune polyglandular syndrome and sarcoidosis where such lymphocytes are seen to accumulate in high numbers.
 |
GD-T cell killing a cancer cell.
(1) A human GD-T (labelled ‘T’) identifies and scans (2) the surface of a cancer cell (labelled ‘C’). On contact with the cancer cell (3) the GD-T releases perforin granules (stained red) into the cancer cell, rupturing its membrane (4) destroying the cancer cell (adapted from – Enc Life Sci, Jul-2007). |
How can GD-Ts be used to treat disease?
Cellular immunotherapy is a form of treatment that harnesses the cells of the immune system to combat disease and is one of the most actively pursued areas of research by biotechnology and pharmaceutical companies today. Interest in immunotherapy is largely driven by recent compelling efficacy data in cancers and by the potential to achieve a cure or functional cure for some patients. While the field of immunotherapy in cancer, in general, has achieved proof of concept and yielded significant durable responses in multiple tumor types, there remain major tumor types such as colon, breast, and prostate cancers as well as patient groups within responsive tumors, that do not respond to current immunotherapy treatments. One theory to explain this non-responsiveness is that certain tumors require direct immune stimulation. T cell-based technologies seek to deliver activated T cells towards malignancies to initiate an immune response. The primary challenges in the field have been to couple an acceptable efficacy and safety profile to successfully target solid tumors.
Adoptive T cell transfer typically involves administration of autologous, allogeneic, or genetically-modified T cells (see footer below) into a recipient host with the specific goal of boosting or transferring enhanced immunologic functionality. One of the most advanced cell-based approaches – chimeric antigen receptor modified T cells (CAR-T) – has gained momentum. In a recent study, patients with refractory B cell acute lymphoblastic leukemia were treated with autologous genetically-modified T cells, with almost 90% of patients showing a marked improvement (Pan et al., 2017). Although the treatment is showing promise for specific tumor types, the safety profile remains a concern, as serious adverse events have previously been reported following CAR-T therapy (Grigor et al., 2017). As a consequence of safety issues related to this approach, regulatory approval may be more complex for this genetically modified T cell therapy which effectively has two ‘starting materials’ – (i) the cellular component, and (ii) a lentiviral vector. The therapeutic premise is well-established – T cells are transduced with a viral vector encoding a chimeric antigen receptor capable of recognizing cancer-specific antigens, for example, CD19 which is commonly expressed on several tumors such as myeloma and B cell lymphomas. Transduction is the process by which DNA is transferred from one cell to another by a virus; in this specific case DNA is introduced via a viral vector (a tool commonly used by molecular biologists to deliver genetic material).
| 56 |
Following transduction, the T cells are genetically primed to recognize and kill specific tumor cells expressing the target antigen. The process involves extracting a patient’s T cells (or growing an allogeneic T cell bank), transfecting the cells with a gene for a chimeric-antigen-receptor (CAR), and re-infusing transfected T cells into the patients. The use of cancer-specific cell therapies has gained momentum as several companies demonstrated that genetically modified CAR-T cells are efficacious when directed against blood tumors. These breakthrough findings have moved cell-based immunotherapy into the forefront of clinical oncology with two drugs now in the market.
T lymphocytes have long been known to play an important role in cancer suppression and modulation of tumor growth and numerous experimental studies have demonstrated the anti-cancer potential of GD-T lymphocytes. Indeed, GD-T cells can recognize a number of specific tumor-associated molecules including non-peptidic antigens (IPP’s – isopentenyl pyrophosphate) and immune surveillance stress signals (such as HSP60/70, MICA, MICB, and ULBP) present on the surface of transformed cells. The GD-T cell overexpresses IL-2 receptors and this cytokine is necessary to activate them (Kjeldsen-Kragh, 1993). On recognizing a tumor cell, GD-T cells exert their anti-cancer properties via release of both perforin and of granzyme, a serine protease which enters the target cell to trigger cell death (apoptosis). Our research efforts are focused entirely on targeting tumors in ways that may result in an improved therapeutic index and that have potential applications in solid tumors as well as hematological malignancies. In contrast to conventional AB CAR-T cells, our GD-T cell technology provides greater specificity in targeting tumors through recognition of IPP-expressing cells, whilst avoiding on-target, off-tumor effects on healthy tissue lacking in IPPs.
Liquid cancers
For cell therapies to be effective several parameters need to be addressed. These include (i) viability, (ii) homing to the tumor, (iii) persistence at the tumor, and (iv) target-specificity.
Use of unmodified GD-Ts to treat blood cancers addresses all the above factors. We believe that (i) we have demonstrated therapeutic cells remain viable when injected into the bloodstream of cancer patients; (ii) our research shows GD-Ts injected into the bloodstream remain in-situ; and (iii) they persist for up to 100 days after administration. Moreover, we believe we have demonstrated that certain late-stage blood cancer patients treated with multiple GD-T doses have shown significantly positive responses. These findings lead TCB to believe that all patients with similar blood cancers may respond to GD-T cell therapy in a positive manner.
Solid cancers
We believe that it may be necessary to use CAR-T technology (i) to maximize therapeutic cell homing into the solid tumor site, and (ii) to increase GD-T cell persistence by ‘tethering’ the cell to antigens present on the cancer cell surface.
In order to overcome toxicities seen with conventional CAR-T approaches, we believe that we have developed a ‘co-stimulatory’ GD-T CAR which will only attack and kill cancerous cells whilst leaving healthy cells unharmed. This is important as many of the current conventional CAR-T therapies cannot distinguish target antigens expressed on healthy cells from those on cancerous cells, which results in various pathologies, including cytokine release syndrome, that in some cases had led to patient death. Such targeting of health cells with conventional CAR-T makes their use in solid cancers difficult, as too much healthy tissue is likely to be destroyed as ‘collateral’ damage in the treatment process.
| 57 |
The diagram below illustrates how TCB’s approach works, using the innate receptors on the GD-T cell surface to act as a ‘safety switch’ – such receptors are generally not triggered by healthy cells, only by disease markers (IPP’s) on the surface of cancerous or virally infected cells.
| A | B |
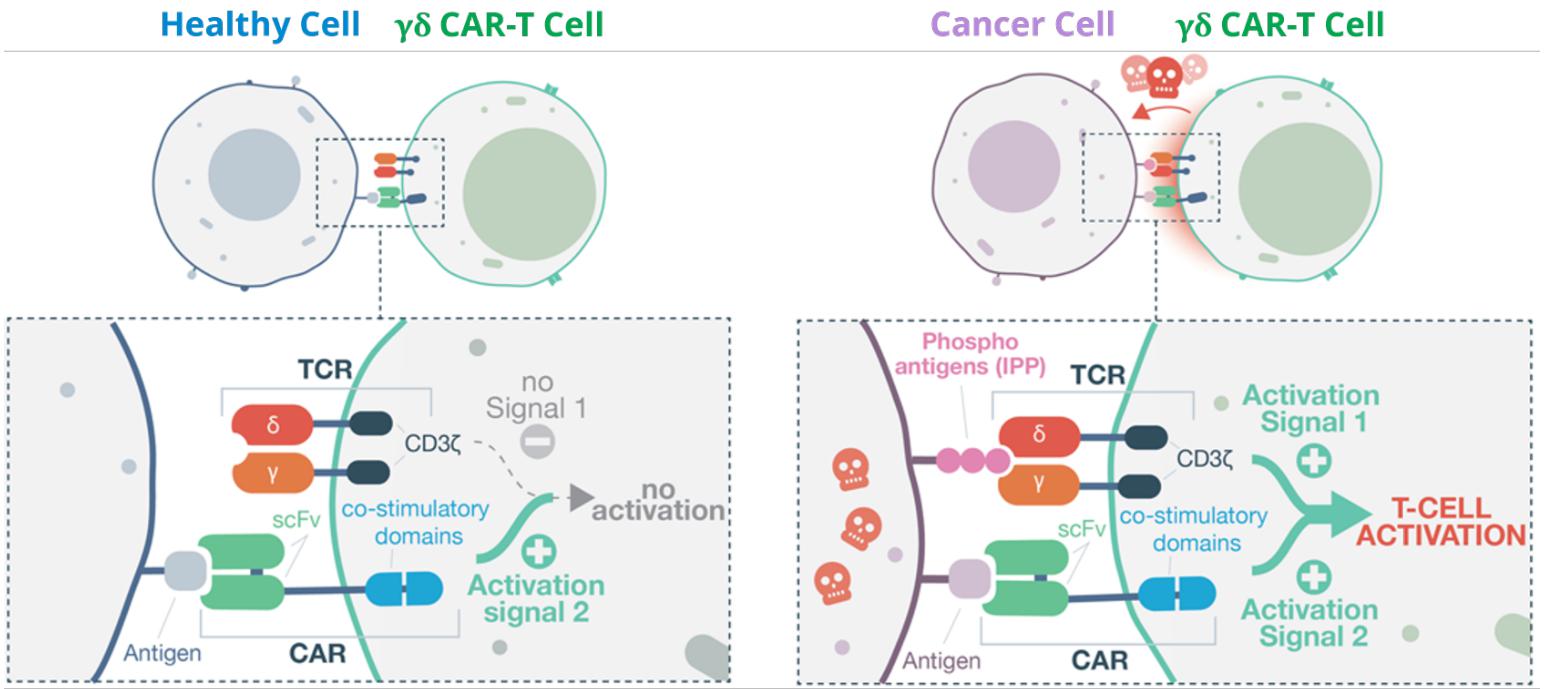
Co-stimulatory CAR-T: A) No GD-T cell activation in healthy cell. B) GD-T activation and cell-killing in cancer cell.
Autologous cells are derived from ‘self’, using patients own cells to treat their specific disease
| 58 |
Allogeneic cells are derived from donor material, giving rise to cell banks able to treat numerous patients
Genetically-modified cells are typically engineered with a ‘chimeric’ receptor to target specific cancer antigens
Commercialization of conventional CAR-T cell therapy has taken decades of high-quality research in academia and industry, and it has provided transformational results for a number of patients with B cell malignancies. However, as noted, there are numerous barriers to widespread adoption, including:
| ● | Severe Toxicities. The significant risk of severe toxicities, especially cytokine release syndrome (CRS) and neurotoxicity occurring up to 3 weeks from treatment. These toxicities have resulted in the need for implementing specific clinical pathways to certify staff and facilities in the administration of the drugs and the management of the toxicities. | |
| ● | On-target, off tumor toxicities. Conventional CAR-T products have no mechanism for discriminating between diseased and healthy cells. Activation is governed solely by the expression of the target antigen, which can lead to toxicity when the target antigen is expressed on healthy cells. In marketed products targeting CD19 (present in the vast majority of B cells), this can be tolerated as B-cell aplasia, albeit with the need for regular long-term immunoglobulin replacement therapy. However, in experimental CAR-T products targeting other antigens this has been shown to cause serious side-effects, up to and including fatality. | |
| ● | Complex supply chains associated with autologous treatments. By definition, autologous treatments require the source cells to have been collected from the patient. It therefore requires a personalized supply chain with multiple touch points and the manufacturing process can only ever be performed on a single-patient batch size. This adds complexity to each treatment and has required the introduction of completely new processes and infrastructure in able to commercialize the products. | |
| ● | Inherent variability of the drug product. Each patient has a different cell population and so the starting material of each manufacturing batch is always variable, leading to variable final product. This can be minimized during pre-screening, which eliminates some patients from treatment, but there are still significant challenges in manufacturing to provide consistent batches of drug products and in understanding which variables are critical to product quality. | |
| ● | High list price of the products. The need for personalized manufacturing, new supply chain processes and management of acute and chronic toxicities have all contributed to the high prices associated with the first CAR-T products reaching the market. In the USA, Kymriah® has a list price of $475,000 for pediatric ALL, and Yescarta® lists at $373,000 for DLBCL patients. The associated treatment costs and ongoing management can increase this price significantly. |
The combination of the co-stimulatory CAR, with GD-T cells, provides TCB with a proprietary platform which we believe addresses the problems with existing CAR-T products in the following ways:
| ● | Using the natural T cell signaling of the GD-T cell will, we believe, result in less risk of hyperactivation and tonic signaling with an overall reduction in the risk of CRS and less exhaustion of the cells. | |
| ● | The requirement on cell activation remains on the endogenous GD-T cell TCR signal, which detects stress signals associated with cancerous cells, so healthy cells are not targeted for destruction even if the target antigen is expressed and the CAR binds, thus off-tumor toxicity is avoided. | |
| ● | Manufacturing in batches of high dose numbers, without the complex patient collection of personalized supply chain steps, we believe will result in a dramatic reduction in cost of goods. This will be reflected in a list price which is in line with current biologicals. With the reduced likelihood of associated toxicities, the treatment and management costs should also be significantly lower, and the products can be made available to many more patients as a result. |
| 59 |
| ● | The combination of a well-tolerated product and simplified supply chain (by virtue of our proprietary CryoTC freeze-thaw process), we believe, will make the therapy suitable for administration in local oncology centers without patients having to locate in centralized specialist centers of excellence, further reducing financial and logistic barriers to treatment. | |
| ● | The tolerance of “off tumor” antigen binding without associated toxicity allows for a complete change in the current target identification paradigm. Instead of identifying targets that are exclusively expressed on tumor cells, we believe our co-stimulatory CAR-T approach confers an advantage to select targets that can be highly expressed on tumors and at low levels on healthy tissue. We select targets based on their relative therapeutic index increase in expression, their homogeneity in tumors and the antigen density. This allows us to target significantly more tumor associated antigens and to significantly expand the therapeutic index into higher doses or repeat administration. | |
| ● | GD-T cells have multiple roles in humans, possessing both innate and adaptive functions. One role is a sentinel surveillance cell, and they are biologically primed to travel through tissue searching for sites of cellular stress. This ability to penetrate tissue makes them advantageous agents for treating solid tumors. We can add additional function to the GD-T cells by using one or more co-stimulatory CAR-T constructs to add targeting to appropriate antigen(s) and to provide armor or strategies to overcome environmental and immune suppression in the tumor microenvironment. Therefore, we believe that the platform offers a promising approach to target the full spectrum of cancer diseases. |
Viral infections
GD-Ts are natural killers of virally infected cells, as well as cancerous cells. We believe that our unmodified GD-T therapy offers substantial potential as a first line of attack against future viral pandemics. During the COVID-19 pandemic, we took the opportunity to develop a trial protocol to treat patients with COVID-19, which was approved by the MHRA. We are currently not progressing this trial because of the absence of available patients given the progression of the disease; however we would consider conducting a phase 1b/2a trial if more severe/pathogenic variants emerge and we believe that there is considerable opportunity to deploy our GD-T therapy in the treatment of viral infections, including rapid response treatment of future epidemics and pandemics and selected acute viral infections. Whilst our current focus is to prioritize cancer treatment we will seek opportunities to develop viral treatments either on our own or in partnership in future Numerous peer-reviewed publications have demonstrated that GD-T cells innate killers of cells which have become virally infected. Using Epstein-Barr virus infected cells as an exemplar, TCB has conducted pre-clinical studies to demonstrate that our GMP-compliant manufacturing process results in GD-T with potent anti-viral cytotoxicity
Autologous versus allogeneic
Commercially available cell therapies typically are either autologous or allogeneic. Autologous products are taken from one donor (the patient) and used to treat that same donor (self-to-self), whilst allogeneic products are usually taken from a single donor (not a patient) and used as the starting material to treat a large number of different individuals (patients). GD-T lymphocytes are known to exert their biological effect in a non-MHC restricted manner. This means the potential for graft-versus-host mediated rejection is significantly reduced if allogeneic (non-self) cells are used as a treatment compared with many other immune cell therapies. As many patients with late-stage cancer or severe viral infections are also immunosuppressed, potential for host-mediated rejection of allogeneic cells is also reduced. When compared with autologous variants, commercial benefits of allogenic treatment include the following:
| ● | significant reduction in cost of goods; | |
| ● | product can be campaign manufactured and stockpiled frozen; | |
| ● | increased capacity to treat more patients; | |
| ● | logistics of shipping product are simplified; | |
| ● | higher doses of (reproducible) product are possible; and | |
| ● | product is immediately available for acute disorders |
| 60 |
Our strategy for developing an allogeneic solution for CAR-T is to select a pathway which will allow us to bring our products to patients as quickly as possible. These concepts build upon decades of previous development in allogeneic cell therapies and have clear understanding of development requirements in terms of manufacturing, clinical and regulatory execution.
Although manufacture of allogeneic cell therapies allows product to be “pharmaceuticalized” by virtue of campaign manufacture and storage, the approach is however not without technical and logistic challenges. To manufacture allogeneic banks, donor cells need to be screened for numerous adventitious agents, including for example, HIV, hepatitis, CMV and syphilis. Additional tumorgenicity testing is required, and assays conducted to ensure the cell bank is free from karyotypic aberrations. In order to overcome any potential for rejection, TCB has developed allogeneic GD-T cell banks that are unlikely to elicit a graft-versus-host (GvH) or host-versus-graft (HvG) immune response.
Donors are screened and selected based on clinically-relevant history and then based on the proliferative capacity and phenotypic character of their GD-Ts, based on a small volume blood draw and in-house assays. In this way, only good quality GD-T cells are selected for repeat apheresis and banking. The banks are HLA-typed and become the starting material for all of the allogeneic CAR-T products. These banks are cryopreserved in our facilities and can later be thawed, genetically engineered with the CAR, activated and expanded into final product, before being frozen again as multiple individual doses of drug product.
Generation of Gamma Delta T cells from IPSC cells
Identification of appropriate donors whilst possible is challenging as only a limited number of batches can be created from a single donation. GD-T cells can be routinely expanded from peripheral blood over 14 days. This provides a short window of opportunity for cell modification/engineering.
Induced pluripotent stem cells (iPSCs) have the potential to overcome these issues because they are capable of unlimited proliferation and multidirectional differentiation. In 2013, several research groups from Japan reported the successful reprogramming of αβT-cells, followed by re-differentiation back to αβT cells (Vizcardo et al., 2013; Nishimura et al., 2013; Themeli et al., 2013). While re-differentiated αβT cells-maintained antigen specificity, they were also characterized by higher proliferation ability than an original T-cell clone.
We hypothesized that GD-T derived iPSCs cells that carry the rearrangements at the TCRG and TCRD gene locus will be able to generate GD-T but not αβT cells. Furthermore, iPSC cells will provide a vast opportunity for the gene-editing without any time constraints of terminally differentiated cells.
Reprogramming GD-T cells has proven to be a challenge, as these cells are not tolerant of cell sorting. Therefore, GD-T cells can be reprogrammed in a bulk culture with the rest of peripheral blood cells or at the end of 14 days expansion, when the purity of GD-T is highest. After several unsuccessful reprogramming attempts, we have optimized the conditions favoring GD-T cells reprogramming. In the last round of reprogramming >50 clones were created. After extensive analysis of DNA rearrangements in δ- and γ-locus of 5 pre-selected clones, it was confirmed that they are derived from GD-T cells with different TCR sequences.
IPSC technology is an attractive approach for the limitless source of GD-T cells are successful progress in reprogramming has been demonstrated. Further work is now required for the establishment of a GMP compatible T-cell differentiation protocol. Generation of GDT cells from iPSC cells presents TCB with a vast opportunity for scaling without any time constraints of terminally differentiated cells.
Fresh versus frozen product
Commercial and clinical development of cellular therapy products will invariably require cryopreservation and frozen storage of cellular starting materials, intermediates and/or final product.
Optimizing cryopreservation is important to obtaining maximum yield and a consistent end-product. Suboptimal cryopreservation can lead not only to batch-to-batch variation, lowered cellular functionality and reduced cell yield, but also to the potential selection of subpopulations with genetic or epigenetic characteristics divergent from the original cell line.
| 61 |
Regulatory requirements also impact on cryopreservation, requiring a robust and reproducible approach to freezing, storage and thawing of the product. This requires attention to all aspects of the application of low temperatures; from the choice of freezing container and cryoprotectant, the cooling rate employed and its mode of delivery, correct handling of the frozen material during storage and transportation, to eventual thawing of the product by the end-user. Each of these elements influences all of the others to a greater or lesser extent and have been taken into consideration as TCB moves from fresh to cryopreserved cell-based product.
In a recent submission to UK regulators, we provided batch manufacture and supporting data, and TCB was granted approval to commence treatment of cancer patients using frozen allogeneic product. This represents a significant milestone for TCB, as we pioneer use of cryopreserved-donated cells to treat cancer and COVID-19 patients. Obvious benefits include increased product reproducibility, ability to ship product globally on request and significant economy of scale (through batch manufacture and storage).
Clinical studies – unmodified GD-Ts in blood cancer
Management of acute myeloid leukemia (AML) is based on intensive chemotherapy and/or stem cell transplant, but these therapies lead to high relapse rates amongst treated patients. Particularly for the relapsed/refractory AML population or those who are not eligible for alloHSCT or intensive chemotherapy, the therapy options are limited, and patients are often placed in experimental protocol therapies or palliative care. As a result, there is a need for additional therapies, particularly for these cohorts.
GD-T cells have emerged as a promising therapy due to their ability to specifically target cancer cells. Nonclinical studies performed in AML cell lines suggest that GD-T cells specifically target AML tumor cells and lead to cell lysis in vitro (Kirk et al., 1993). Additionally, in xenotransplantation animal models, GD-T cells obtained from healthy volunteers specifically target AML cells and result in increased survival and diminished tumor burden in NOD mice (Gertner-Dardenne et al., 2012). Similarly, in vitro experiments conducted by TCB further support such findings whilst providing evidence that OmnImmune® (TCB002) specifically targets stress induced cells and effectively kills AML cells lines.
In the clinic, allogeneic treatment in AML patients in the phase 1b/2a trial OmnImmune® (TCB002) has shown our product is well-tolerated with some preliminary evidence of anticancer activity. Firstly, there were no signs of graft vs. host disease (GvHD) following therapy and secondly, CR (complete response) and MLFS (morphologic leukemia free state) were observed. Earlier results with autologous product demonstrated good tolerability. For the allogeneic product, OmnImmune® (TCB002), additional procedures were included to prevent GvHD (e.g. AB T cell depletion). Literature reports were also supportive of the use of OmnImmune® (TCB002) in cancer patients. The phase 1b/2a trial tested OmnImmune® (TCB002) in active relapsed or refractory AML who were not eligible for or did not consent to high dose salvage chemotherapy and/or allogeneic hematopoietic stem cell transplantation (alloHSCT). The trial was conducted to identify a tolerable dose and better understand the safety of this therapy in the chosen indication as well as generate preliminary information on potential clinical benefit. The primary, secondary and exploratory endpoints were as follows:
Primary endpoints:
| ● | Assessment of adverse events (Aes) graded by Common Terminology Criteria for Adverse Events (CTCAE) v5.0, vital signs and evaluation of laboratory parameters | |
| ● | Incidence of dose-limiting toxicities (DLTs) during the first 28 days after γδ T cell administration. | |
| ● | Establish Maximum Tolerated Dose (MTD) of OmnImmune® |
Secondary endpoints:
| ● | Complete Remission (CR) rate |
| 62 |
| ● | Overall survival (OS) | |
| ● | Quality of life determined by EORTC QLQ-C30 questionnaire |
Exploratory endpoints:
| ● | Changes in γδ T cell count and phenotype before and after OmnImmune® infusion |
No formal statistical analysis was planned. The incidence of DLTs were to be summarized descriptively by γδ T cells dose for evaluable patients. The recommended dose would be determined as the greatest with an incidence of DLTs no greater than 1/3. All other data including efficacy results were summarized descriptively by γδ T cells dose.
The trial enrolled 8 patients and healthy donors aged >18 years.
Clinical outcome
Seven patients were treated with OmnImmune® (TCB002). The eighth patient could not be dosed because the study was terminated as a result of the COVID-19 pandemic, which prevented the importation of investigational product from Scotland to the Czech Republic. No safety concerns were raised during Safety Review Committee (SRC) meetings. No treatment related Serious Adverse Reactions (SARs) were reported in any of the patients who were enrolled in the trial. No grade 3≥ OmnImmune® (TCB002) treatment related toxicities were noted in any of the treated patients. No dose-limiting toxicities were observed and no emergency safety measures have occurred for any subjects receiving OmnImmune® (TCB002). Two patients at 28 days post-treatment achieved a CR (one patient) or MLFS (one patient); another patient was classified as attaining stable disease with > 50% reduction in bone marrow blast count; one additional patient exhibited reduction in blast levels at 14 days; and one patient had disease progression (see table below). One patient (PRA1-5003) died 21 days after TCB002 due to bilateral pneumonia, determined unrelated to study medication. One patient (PRA1-5010) was withdrawn because of the COVD-19 pandemic before bone marrow aspiration on day 28 post-treatment. These preliminary indications of anticancer activity were not expected given the refractory profile of the enrolled patients.
The EORTC QLQ-C30 questionnaire resulted in scoring from six of the seven patients dosed with OmnImmune® (TCB002) for varying periods of time depending on their study duration. At 7 days post dosing, the average QoL score from six patients had decreased from 55.7 to 47.2 out of a possible maximum of 100. This negative impact on QoL reflects the well characterized side effects of preconditioning therapy with cyclophosphamide and fludarabine given between 6 and 2 days prior to OmnImmune® (TCB002) administration. The score remained lower in the four patients assessed at 28 days at a level of 50.0. In the two patients (one CR and one MLFS) who were assessed at the end of the study (week 24), both had recovered to an improved QoL score, each of 67.0.
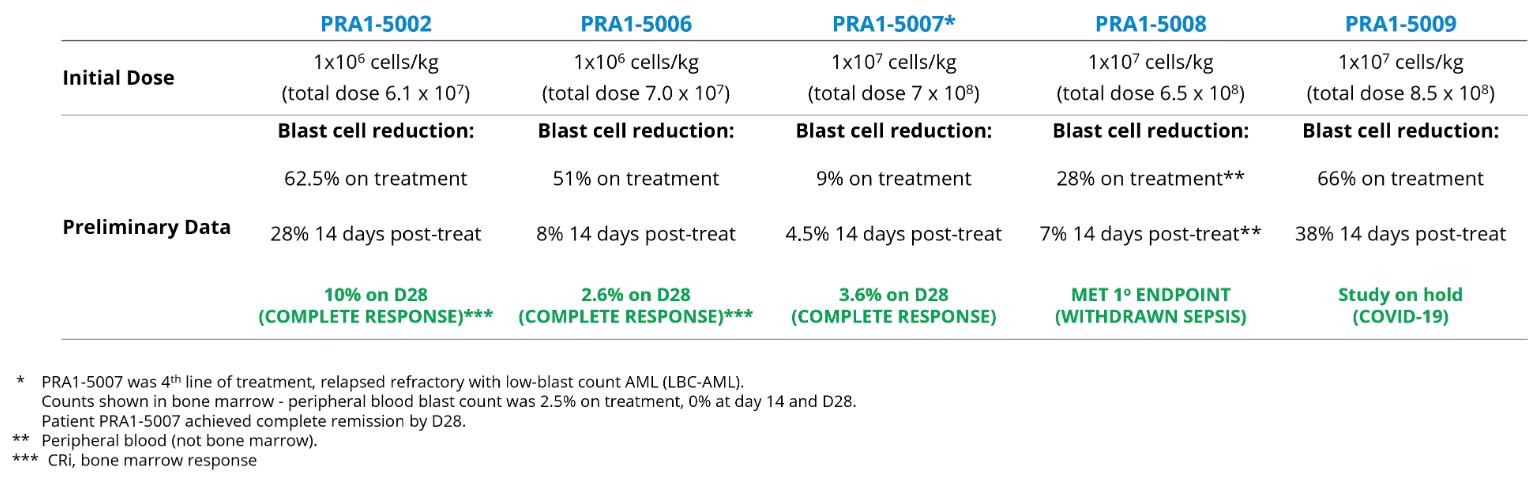
FDA Orphan Drug Designation
About 60 million people living in the European Union (EU) and USA suffer from a rare disease. The European Medicines Agency (EMA) and FDA play a central role in facilitating the development and authorization of medicines for rare diseases, which are termed ‘orphan medicines’ in the medical world. Developing medicines intended for small numbers of patients has little commercial incentive under normal market conditions. Therefore, the EU and USA offer a range of incentives to encourage the development of designated orphan medicines.
The general therapeutic strategy for the treatment of AML has not changed substantially over the past 30 years. Excluding APL (which should be treated with trans-retinoic acid), AML management is based primarily on induction, incorporating an anthracycline and cytarabine, and consolidation therapy, and/or allogeneic Hematopoietic Stem Cell Transplantation (alloHSCT). Induction/consolidation therapy leads to high CRs rates in those who are eligible for treatment and present a favorable risk profile.
| 63 |
Several novel agents are in various stages of development for the treatment of AML. Novel approaches include antibody-based immunotherapy and adoptive cell therapy that aim to improve anti-leukemia T cell function, such as the therapies developed by TCB (OmnImmune®).
OmnImmune® (TCB002) was initially studied in patients with active relapsed or refractory AML who are not eligible or do not consent to high dose salvage chemotherapy and/or alloHSCT. In July 2019, OmnImmune® (TCB002) was granted ‘orphan medicine’ status from the FDA for Acute Myeloid Leukemia (AML). TCB intends to conduct a further clinical phase 2/3 study (OmnImmune® (TCB008-001)) in 2021/2 aimed at treating earlier stage AML patients.
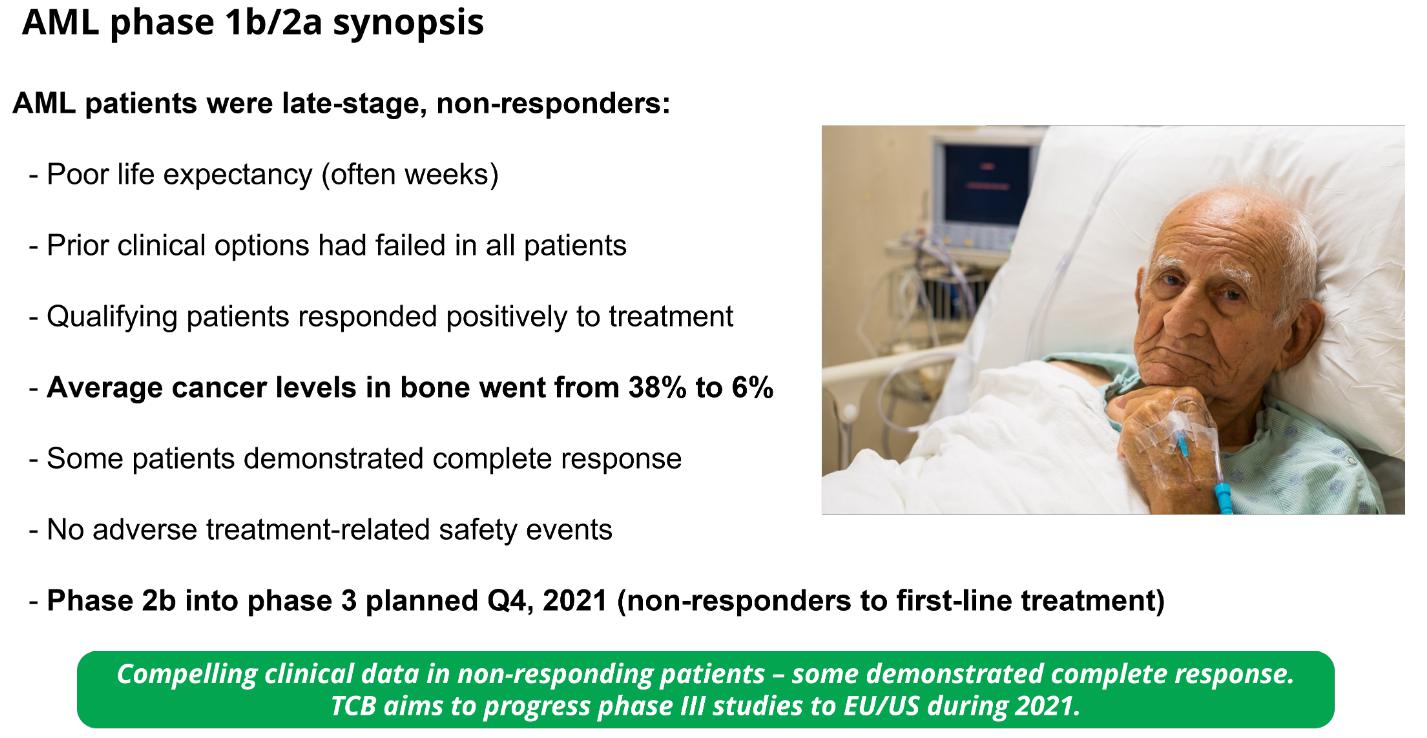
Summary of TCB’s phase 1b/2a clinical trial in patients with fourth-line-of-treatment acute myeloid leukemia. Following completion of the study, TCB plans to commence phase 2b into 3 (pivotal) patient treatment during H1, 2022.
Pipeline and plan
Our future pipeline is focused on treating liquid cancers with our unmodified GD-T therapies and the treatment of solid cancers with next-generation allogeneic GD-T CAR-T therapies.
Our unmodified cell therapy, used in the treatment of Acute Myeloid Leukemia, is supplied under the name OmnImmune.
OmnImmune® is an allogeneic unmodified GD-T (GD-T2) cell product. Donor-derived GD-T cells for proliferative capacity, were activated and expanded in our manufacturing facility before being infused into the patient as part of our OmnImmune® (TCB002) phase 1 trial. This trial was completed in H1 2020 at the Institute of Hematology and Blood Transfusion in Prague, Czech Republic. Having generated meaningful clinical data showing our product is well-tolerated in late-stage AML patients with no remaining treatment options, TCB aims to commence phase 2b-into pivotal (phase 3) clinical studies (with OmnImmune®) during 2022 in AML patients who have failed to respond adequately to induction therapy. The aim is to provide a form of salvage therapy which will either stabilize the patient, thereby preventing disease progression, or delay the requirement for human stem cell transplant. Our initial trial centers will be in the UK, and we anticipate treating our first patients in Q2 2022. Working on the premise that other blood cancers should respond to GD-Ts in a similar manner to AML, TCB plans to conduct clinical studies for OmnImmune® in other hematological malignancies in future. The initial phase 1b/2a trials were undertaken using fresh cell-based product under the program number TCB002. For ease of reference, when discussing that specific trial, we refer the program as OmnImmune® (TCB002). The subsequent planned phase 2b-into pivotal (phase 3) clinical studies will use a frozen cell-based product under the program number TCB008-001. When discussing that specific trial, we refer the program as OmnImmune®.
| 64 |
We plan to develop a range of allogeneic co-stimulatory GD-T CAR pre-clinical drug candidates which will target antigens expressed on a number of solid tumor types.
TCB has generated in-vitro preclinical data as part of our CAR-T program which demonstrated that GD-Ts are very high purity and can be CAR-transduced with high efficiency (see diagram below). Gamma delta cell purity and transduction efficiency have been measured using flow cytometry. CAR positive cells were measured by a detection reagent labelled with the fluorophore Phycoerythrin (PE). Flow cytometry analysis used the parameters of side scatter height (SSC-H) and PE area (PE-A) to define the cell populations. This is demonstrated in the figure below comparing non-transduced (NTD) and transduction with a co-stimulatory CAR construct (co-stim CAR).
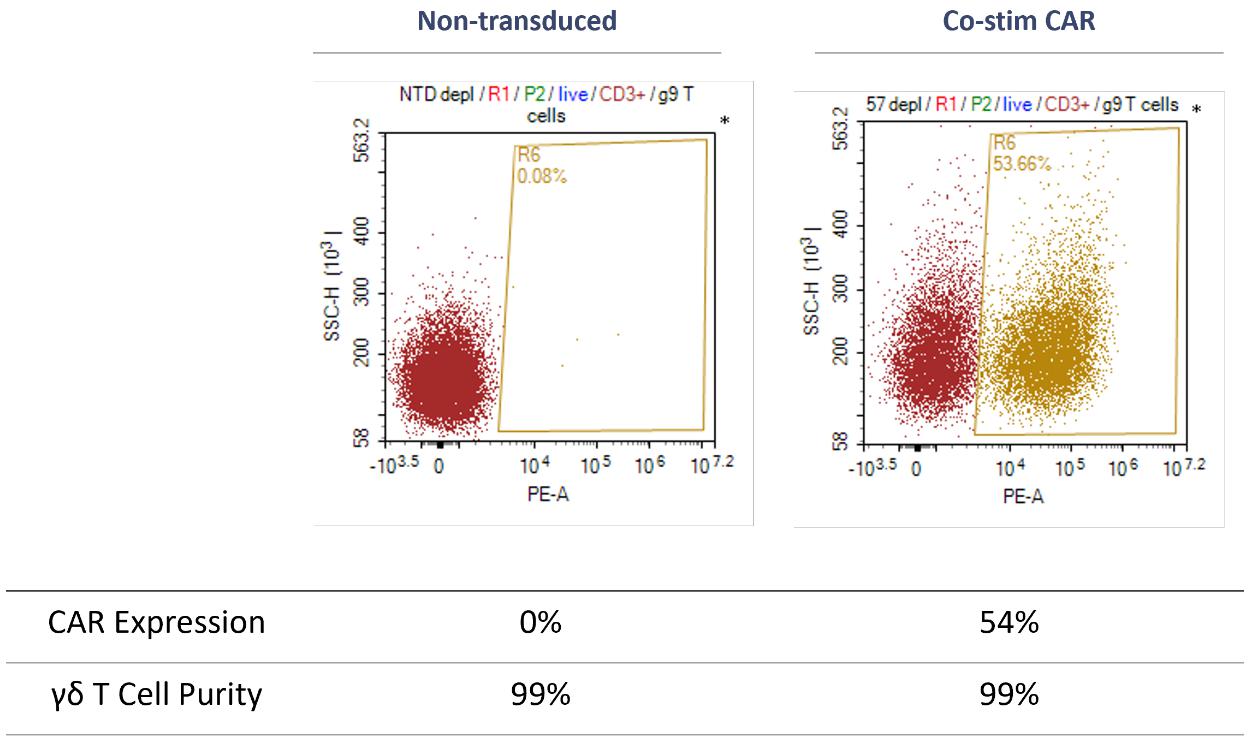
We have also demonstrated that following transduction with different CAR constructs, GD-T’s can be effectively and reproducibly expanded in-vitro whilst exhibiting increased cytotoxicity in a zoledronate-dependent manner (see diagrams below – zoledronate-dependency reflects TCB’s proprietary process for commercial expansion of GD-T’s). The CAR constructs contained different endodomains including DNAX-activating protein 10 (DAP-10) and the high affinity IgE receptor (FcR) with no endodomain (no-endo) and non-transduced (NTD) as controls. These data outline the key preclinical parameters investigated in advance of progressing our CAR-T products into clinical trials. TCB has engaged with UK regulators to discuss the design of GD-T CAR phase1b/2a clinical studies (specifically relating to patient dosing and quality systems).
| 65 |
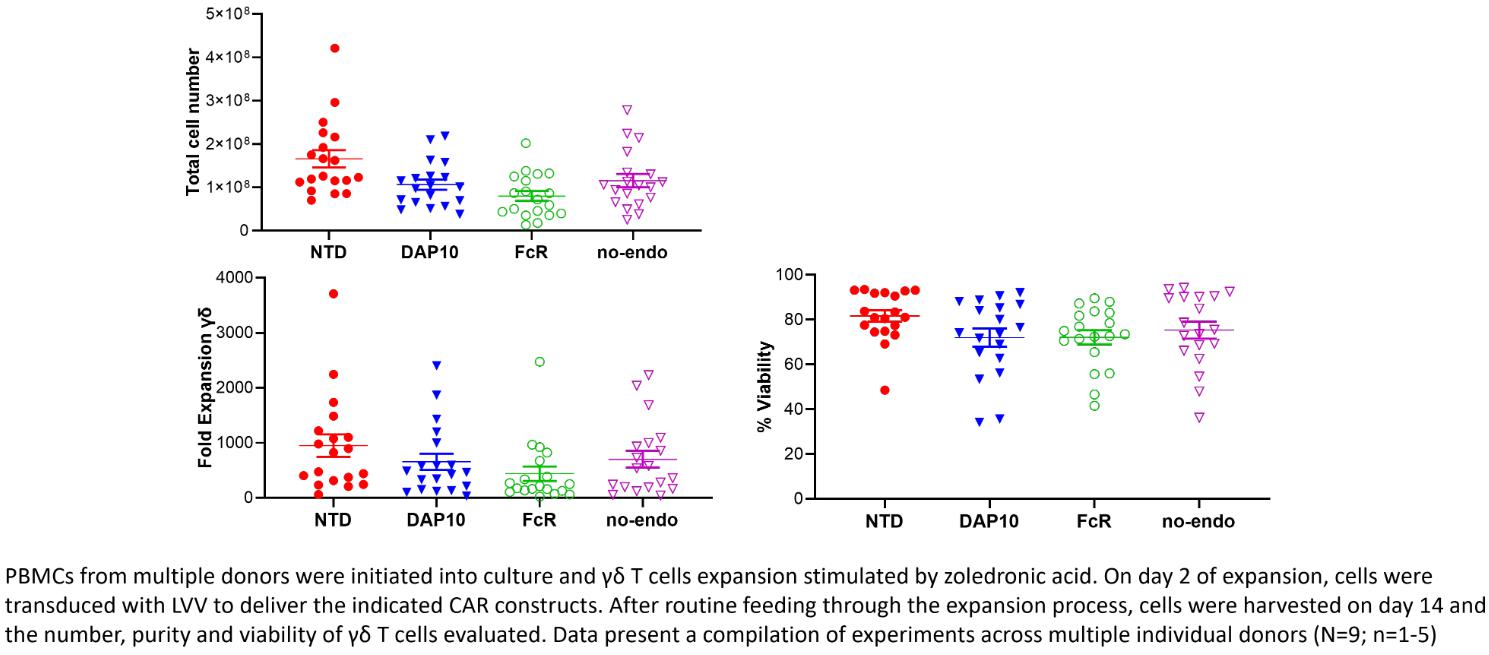
Peripheral blood mononuclear cells (PBMCs) were initiated into culture and GD-T cells expansion stimulated by zoledronic acid. On day 2 of expansion, cells were transduced with lentiviral vectors (LVV) to deliver the indicated CAR constructs. After routine feeding through the expansion process, cells were harvested on day 14 and the total cell number, fold expansion and viability of GD-T cells evaluated. Data present a compilation of experiments across multiple individual donors (N=9; n=1-5).
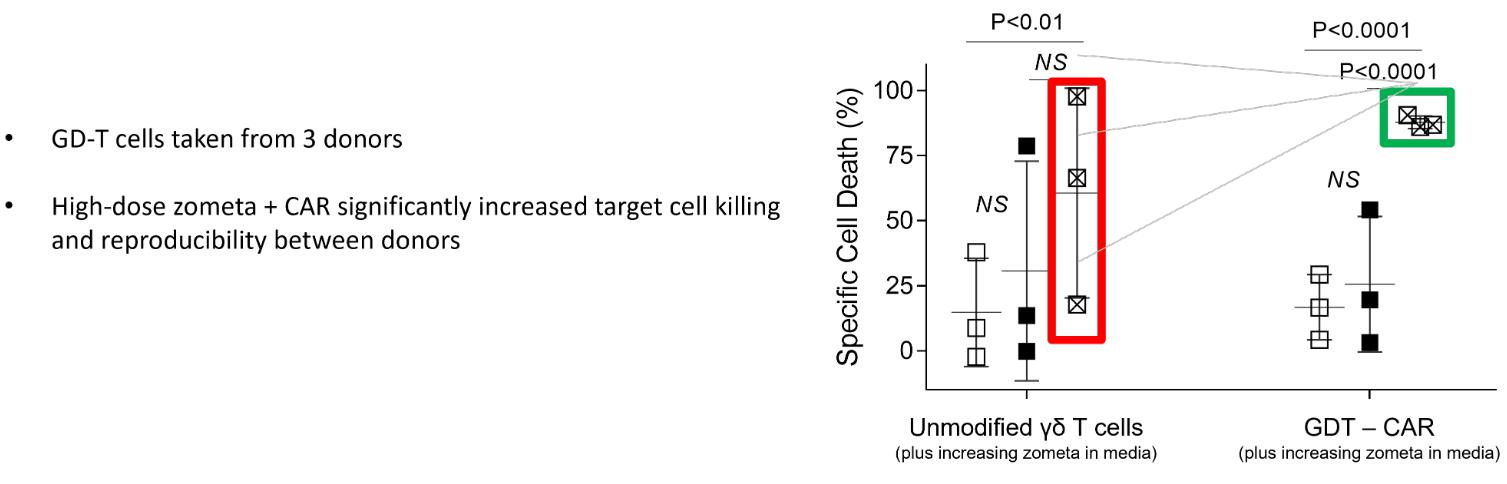
Manufacturing
Unlike many pre-clinical and early clinical stage biotech companies that rely on outsourcing key manufacturing and development functions with consequent complex and expensive supply chains and delays in delivery and execution, we have built a world-class fully integrated GMP grade specialist GD-T manufacturing center in Glasgow, Scotland. This facility undertakes all key functions associated with our GD-T cell development, testing, quality assurance, product manufacture, clinical trial recruitment, management design, support and interaction with regulators. This has resulted in rapid, focused development; highly efficient cost control;, controlled supply chain; speed of development and clinical delivery. We employ over 80 highly qualified people at our facility. The inspiration to create a fully integrated facility came from our founders’ vision and considerable experience in cell therapy.
All advanced therapy medicinal products in the UK must be manufactured by law under a manufacturer’s license granted by the MHRA. TCB received its Manufacturer’s Authorisation for Investigational Medicinal Products MIA (IMP) from the MHRA in January 2015 (license number MIA (IMP) 42803). In April 2016, the MHRA granted the ‘Specials’ license to TCB as well as approving the facility for ongoing GMP compliance, which permits the manufacture and release of Advanced Therapy Medicinal Products (ATMPs) for use in clinical trials.
| 66 |
The backbone of our company is TCB’s Quality Management System, which TCB based on the principles of the current GMP as described in the ‘Rules and Guidance for Pharmaceutical Manufacturers and Distributors’ and EudraLex Volume 4 as revised. This is achieved by the application of a Quality Management System based around the requirements of ICH Q10 and the EU GMP Guide, which address factors affecting the desired quality, namely the personnel, facilities, equipment, materials, processes, procedures training, vendor selection and approval, User Requirement Specification (URS) qualification and validation of assays and systems and the record keeping. All personnel joining TCB undergo rigorous training on everything from GMP through to formalized systems for measuring and evaluating risk.

*MHRA approved GMP compliant (last inspection December 2020 – observations only)
TCB’s manufacturing facilities are equipped with two Class B clean rooms with space secured for future expansion for production of our products as it progresses from phase I to phase III clinical trials. The facility is also equipped with Development and Quality control testing laboratories together and ample stores for goods inwards and product release plus storage for intermediate and final product. Equipment is controlled and monitored through a Management Information System with 24/7 monitoring. All laboratory equipment undergoes a formal URS and once installed undergoes full qualification prior to it being put into routine use.
TCB’s Quality Control team are responsible for the majority of release testing for our products. The Quality Control departments (analytical and microbiology) are responsible for product characterization using bespoke phenotyping and potency assays, safety testing assays and final release of the product to the clinic. In-house testing within TCB’s Quality Control laboratories eliminates the necessity for third party involvement, resulting in reduced costs and gaining full control of scheduling. The Quality Control departments remit also extends to the microbiological monitoring of the facility to measure, assess and control the exceptionally high levels of sterility required within the aseptic manufacturing suites. Extensively equipped Quality Control microbial laboratories allow environmental monitoring of the manufacturing cleanrooms to GMP standards. The laboratories house incubators, biological safety cabinets, centrifuges, fridges, freezers, air and particle monitors.
| 67 |
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe that our scientific knowledge, technology and development experience provide us with competitive advantages, we face potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions, governmental agencies and public and private research institutions. Any GD-T cell therapeutic candidates that we successfully develop and commercialize will compete with existing products and new products that may become available in the future. We believe our advanced clinical products in allogeneic and unmodified GD-Ts provide us a first mover advantage in oncology and viral indications. Our continued efforts in advancing our modified platform technologies, along with our efforts in banked GD-Ts, are in direct competition with a number of public and private companies in the cell therapy space.
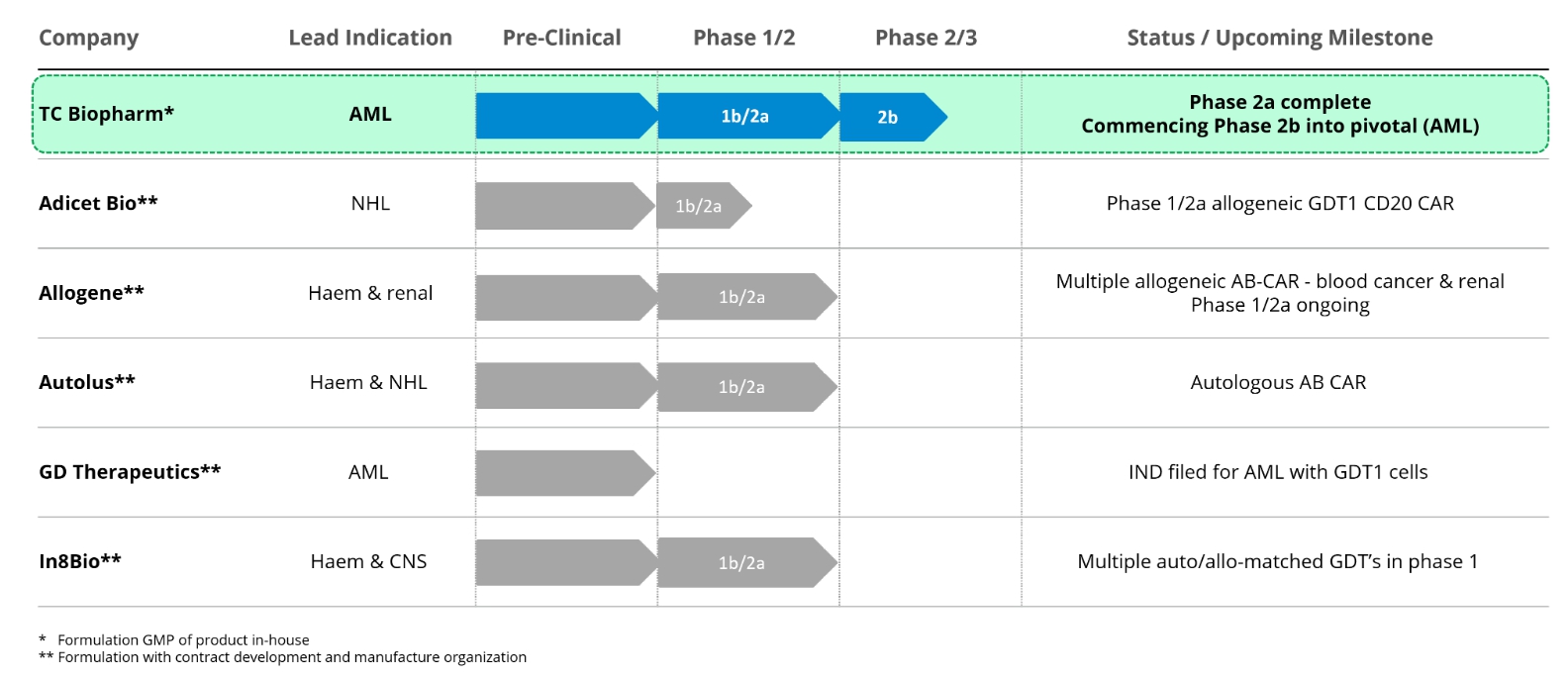
TC BioPharm is part of a growing number of companies commercially active in the cellular immunotherapy space. Such companies developing call-based products include AdicetBio who recently presented phase 1 data from patients with non-Hodgkin lymphoma using allogeneic GDT-1’s modified with a CAR against CD20 – published initial results documented safety and CR/PR in some patients. Other companies include Allogene who are using various CAR-modified allogeneic alpha-beta cells to treat non-Hodgkin lymphoma, multiple myeloma, acute myeloid leukemia and renal cell carcinoma; Autolus who are conducting two phase 1 clinical studies using autologous alpha-beta T cells using CAR’s directed against either CD19/22 or CD20, listed indications include acute lymphoblastic leukemia, B cell non-Hodgkin lymphomas and chronic lymphoblastic leukemia; Gamma Delta Therapeutics who are developing a GDT-1 variant for hematological malignancies, IND filed; and In8Bio who have several ongoing phase 1 clinical programs including an autologous DRI resistant to alkylating agents for treating glioblastoma and an allogeneic product for treating patients with acute leukemia, In8Bio also have a bespoke GDT therapy for AML derived from hematopoietic stem cell transplantation. Apart from TCB who manufacture cell-based product in-house, we believe the above companies contract-out GMP formulation of clinical product to third-party organizations.
| 68 |
Commercial leaders in the CAR-T space are Novartis AG (Basel, Switzerland) and Gilead (Foster City, CA). Both of these companies market autologous CD19-targeted AB CAR-T products. Bristol Myers Squibb (New York, NY) is looking to gain approval for its CD19-directed CAR-T before the end of 2020. Via third party collaborations, all three of the commercial leaders in autologous CAR-T, have accessed gene editing technology with a view to creating allogeneic products. Novartis have partnered with Intellia (Cambridge, MA), Gilead have an agreement with Sangamo Therapeutics (Richmond, CA) and Bristol Myers Squibb have an agreement with Editas Medicine (Cambridge, MA).
We do not believe that any of these competitors will offer the same commercial proposition as our GD-T cell therapeutic candidates due to our:
| ● | Ownership of foundation IP of the co-stimulatory CAR technology within GD-Ts. | |
| ● | First-mover advantage in the field of modified GD-Ts as therapeutics. | |
| ● | Ability to GMP manufacture large numbers of modified GD-T cells to a high purity in a cost-effective manner. | |
| ● | Established banks of allogeneic products which may be used in future (following appropriate regulatory approvals) to treat both cancer and severe viral disease. | |
| ● | The potential to create CAR-T therapies with significantly improved safety profile, suitable for widespread market adoption. | |
| ● | Experience of, and in-house management of, our clinical trial programs. | |
| ● | Pipeline development strategy and screening tools to develop a deep pipeline of platform products for a range of diseases. |
Our Strengths
Our clinical trials have provided very strong evidence of drug-toleration and some preliminary evidence of clinical benefit.
Our clinical trial of TCB001 involved treatment of patients with autologous unmodified GD-Ts. In a phase 1b/2a dose-ranging safety study (maximum total dose 30x109 cells) we saw no evidence of drug-related severe adverse events. A total of eight patients were treated with escalating doses of TCB001, and no treatment-related toxicities were reported during the full six-week therapeutic course. Data from OmnImmune® (TCB002) suggests an excellent tolerability, with no observed Host versus Graft Disease (HvGD) and some preliminary indication of clinical benefit. OmnImmune® (TCB002) has been granted Orphan Drug Designation by the FDA.
Our CAR-T platform is centered on development of safer and more widely applicable therapeutic candidates and associated process and manufacturing capabilities.
Our proprietary co-stimulatory CAR-T technology platform covers identification of target cancer antigens, successful design and engineering of target sequences, preclinical safety testing and optimized manufacturing processes suitable for producing therapeutic candidates for use in clinical trials and commercialization. We believe the platform will enable development of additional GD-T cell therapeutic candidates targeting cancers that have previously been difficult to treat. We believe the products will be demonstrably safer than the current generation of AB T cell CAR-T products because they will not attack healthy non-cancerous cells and augment the natural biological process rather than bypassing it.
| 69 |
We have identified a large and growing pool of cancer targets for which we can develop additional therapeutic candidates.
We have identified over 20 antigens that are preferentially expressed in cancer cells and have established ongoing research programs to develop several of these into our GD-T platform. Within the terms of our agreement, bluebird bio, we have first right of refusal on a further three oncology targets. Each antigen target presents an opportunity to target many cancer types and therefore presents multiple potential represents a development, collaboration and/or an out-licensing opportunity as each target could be used to target specific cancer types. Growing the pipeline of products built on our co-stimulatory CAR-T and reaching patients is our priority.
We have historically entered collaborative arrangements with partners (bluebird bio, Inc (now 2seventybio). (USA) and Nipro Corporation (Japan), which involve funded or partly funded preclinical collaboration. It is uncertain at this time whether TCB will receive any significant revenues from these collaborations.
We retain control of key business elements, such as product manufacture and clinical research.
Whilst many companies contract out product manufacture, quality systems and clinical trial management, we have elected to build these skills in-house. TC BioPharm has a GMP (Good Manufacturing Practice) cleanroom facility where our products are manufactured. We also retain all the quality support systems such as product testing and release of final product to the clinic. Keeping these systems in-house allows the Company to control all aspects of the manufacturing process whilst significantly reducing costs of goods (CoGs). Further saving on costs are accrued by in-house manufacture, as contract manufacturing organizations (CMOs) will typically charge several times more than the actual costs to maintain their profit margins. Rather than fully outsource our clinical trial management, data management and pharmacovigilance, we maintain an inhouse clinical team that partners with a contract clinical research organization (CRO) for data management and pharmacovigilance services. The inhouse clinical team conducts and manages our own clinical trials in-house. In addition to significant cost savings, this allows us to build a strong working relationship with physicians who are treating the cancer patients; we believe this is key to successful product development as the physicians participating in our clinical studies will also be our future customers. We believe that retaining control of key elements of our business such as GMP manufacture and clinical operations, has allowed TC BioPharm to move quickly and efficiently since incorporation.
We continue to file new patent applications from new in-house product development, and have a strong growing intellectual property portfolio to protect our products and proprietary platform.
We have a strong intellectual property portfolio covering the key aspects of our manufacturing processes and product platforms. Our in-house product development team consists of 14 scientists who are dedicated to developing new therapeutic candidates and optimizing current manufacturing processes. All of our patent families are currently in various stages of the patent approval process, and as leaders in the path towards the commercialization of GD-Ts we hold significant first-mover advantage captured by trade secrets and know-how.
Our policy of developing strategic alliances has and will provide additional support for product development and commercialization.
We believe that strategic alliances, both historic and potential future alliances, have and will provide extensive experience in scale-up and automation, culture media manufacture and post-authorization sales and marketing with regional expertise. Additionally, we expect to use knowledge gained from our collaborations to improve development pathways for our unpartnered CAR-T therapeutic candidate programs.
We have a highly knowledgeable and experienced management team with extensive industry experience and expertise in the United States and in Europe.
Our senior management has substantial experience in the biopharmaceutical industry, including our Executive Chairman and co-Founder, Dr Michael Leek, who has 30 years’ experience of commercial regenerative medicine, serving on senior management teams and boards of public and private companies in the biotechnology sector, including several years as a founding director of Intercytex – a UK-based cell therapy company which listed on AIM in 2006. Mr. Kobel joined us as our Chief Executive Officer at the time of our IPO. Bryan brings a US presence to our executive team and over 15 years’ experience in Healthcare and Life Sciences capital markets. Our Chief Operating Officer and co-founder, Angela Scott, has 38 years of experience in cancer research and commercial biotechnology, working across several disciplines including preclinical and clinical development plus GMP manufacture; she was also one of the small team directly responsible for cloning Dolly the Sheep at PPL. Martin Thorp, our Chief Financial Officer has over 30 years’ experience in implementing capital strategies globally from seed investment to IPO. He was global CEO of Arthur Andersen Corporate Finance based in New York.. Dr Sebastian Wanless, who heads our clinical and regulatory team, has over 30 years industry experience in clinical research and medical affairs. Sebastian was VP of Intercontinental Research at Bristol-Myers Squibb in the United States with international experience in Europe and Japan.
| 70 |
Ability to treat patients under the ‘Specials’ regulatory framework.
European regulations (Regulation 167 of the Human Medicines Regulations 2012) set out the exemption from the requirement for a medicinal product, placed on the market in the UK to hold a marketing authorization. This exemption flows from Article 5(1) of EU Directive 2001/83/EC, which states that a member of the EU may, in accordance with legislation in force and to fulfil special needs, excludes from the provisions of this Directive medicinal products supplied in response to a bona fide unsolicited order, formulated in accordance with the specifications of an authorized healthcare professional and for use by an individual patient under his or her direct personal responsibility. Such an unlicensed medicinal product may only be supplied in order to meet the special needs of an individual patient. An unlicensed medicinal product should not be supplied where an equivalent licensed medicinal product can meet the special needs of the patient. Responsibility for deciding whether an individual patient has “special needs” which a licensed product cannot meet should be a matter for the doctor, dentist, nurse independent prescriber, pharmacist independent prescriber or supplementary prescriber responsible for the patient’s care.
In 2016 we were granted ‘Specials’ License by the UK Medicines and Healthcare Regulatory Agency (MHRA). We have embraced the opportunity for broadening patient population by treating individual patients with different tumor types through a ‘Specials’ License. Clinicians have expressed strong initial interest in treating patients with solid tumors; along with blood-borne tumors such as multiple myeloma, chronic myeloid leukemia (CML) and chronic lymphocytic leukemia (CLL) with OmnImmune®.
In terms of time and cost, the ‘Specials’ scheme is an attractive strategy. We believe that accumulating evidence by this route could lead to rapid and wider product uptake through ‘off-label’ use.
Intellectual Property
We have a strong portfolio of patents covering manufacture and commercialization of GD-T cell products and their modification via CAR-T (summarized below). Our technology platform and clinical programs have enabled us to raise over $50 million in grant, equity and collaboration funding since becoming operational in 2017. This financing has allowed us to enhance and expand our clinical and preclinical programs as well as build our team of world-class scientists.
The following table provides an overview of our core technology platforms, technology assets and competencies across the business. Additional details of our intellectual property portfolio are provided below.
| ASSET SUMMARY | ATTRIBUTES | ||
| GD-T Vehicle | ● | Readily available and expanded to high numbers. | |
| ● | Not MHC-restricted, therefore no graft vs host disease – an allogeneic platform. | ||
| ● | Pre-programmed tropism for infiltration of diseased tissue. | ||
| ● | Multiple modes of innate cytotoxicity and coordinating a wider immune response. | ||
| ● | Clinical tolerability of the allogeneic vehicle demonstrated at high dose level. | ||
| ● | Naturally arising in different subtypes offering a menu of vehicles with unique properties. | ||
| 71 |
| Allogeneic Cell Banks | ● | Donor GD-Ts selection based on highest therapeutic quality. | |
| ● | Reproducible product with low cost-of-goods compared with autologous (patient-bespoke) therapies, can be frozen-shipped, thawed at clinic. | ||
| ● | Well understood clinical and regulatory pathway to commercialization. | ||
| Co-stimulatory CAR-T | ● | Elimination of off-tumor toxicity. | |
| ● | Reduction of cytokine release from killing healthy cells. | ||
| ● | Reliance on natural T cell activation and no tonic signaling | ||
| ● | Antigen expression on healthy tissue tolerated – greatly expanded range. | ||
| ● | Ability to use multiple co-stimulatory receptors to add functionality. | ||
| Integrated Business Model | ● | Full control of critical stages of development projects, which increases speed and reliability of development and production, optimizes operations to our specialized products and materially reduces our cost base | |
| ● | No pass-through or transaction costs form external service providers, which increases efficiency and speed of development and manufacturing and materially reduces our cost base | ||
| ● | In-house clinical management ensures best chance of clinical success and avoids use of very expensive clinical management in early-stage trials, materially reducing our cost base. |
The strength of our patents involves complex legal and scientific questions and can be uncertain. We currently own over 60 pending patent applications worldwide.
We actively seek to protect the intellectual property and proprietary technology that we believe is important to our business, including seeking, maintaining, enforcing and defending patent rights for our therapeutics and processes, whether developed internally or licensed from third parties. Our success will depend on our ability to obtain and maintain patent and other protection including data/market exclusivity for our therapeutic products and platform technology, preserve the confidentiality of our know-how and operate without infringing the valid and enforceable patents and proprietary rights of third parties.
Our policy is to seek to protect our proprietary position generally by filing an initial priority filing at the U.K. Intellectual Property Office, or UKIPO. This is followed by the filing of a patent application under the Patent Co-operation Treaty claiming priority from the initial application(s) and then progressing to national applications in, for example, the United States, Europe, Japan, Australia, New Zealand, China and Canada. In each case, we determine the strategy and territories required after discussion with our patent professionals to ensure that we obtain relevant coverage in territories that are commercially important to us and our GD-T therapeutic candidates. We will additionally rely on data exclusivity, market exclusivity and patent term extensions when available, including as relevant exclusivity through orphan or pediatric drug designations. We also rely on trade secrets and know-how relating to our underlying platform technology and therapeutic products. Prior to making any decision on filing any patent application, we consider, with our patent professionals, whether patent protection is the most sensible strategy for protecting the invention concerned or whether the invention should be maintained as confidential.
As of December 1, 2021, we owned 2 granted patents and 48 patent applications in 6 families, and have an exclusive license to an additional 1 family of 1 granted patent application and 13 patent applications. Consistent with the filing strategy outlined above, all of our applications are either UK applications, PCT applications or national phase applications derived from a corresponding PCT application. All sets of national phase applications include a US application. These patent applications include claims directed to our therapeutic products and platform technology or other manufacturing and process technology to further enable our therapeutic products and manufacturing methods.
WO 2016/166544 (Modified Gamma Delta T Cells and uses thereof). International filing date April 14, 2016, earliest priority date April 15, 2015.
| 72 |
We own a patent application covering a method of treatment for cancer using GD-T cells that express chimeric antigen receptors (CARs). The patent application claims are directed to GD-T cells expressing a co-stimulatory CAR, the advantages of the co-stimulatory CAR by inhibiting on-target, off-tumor activation due to its design, to the method and process of modifying a GD-T cell to express the co-stimulatory CAR, and to medical uses of the modified GD-T cell. Application has issued as a granted patent in the US (US 10881688 B2, expires October 7, 2036). Application has been allowed in Israel (IL 255011), the statutory opposition period has now elapsed with no opposition proceedings being raised, and we expect to receive notification of grant in due course. Applications have been allowed in Japan (JP 2017-554035) and grant in South Africa we expect to receive notification of grant shortly. National applications remain pending in: Australia, Brazil, Canada, China, Hong Kong, Japan, South Korea, New Zealand, Singapore, the US. Regional applications are pending before the European and Eurasian Patent Offices.
WO 2016/174461 (T cell which expresses a Gamma Delta T cell receptor and a Chimeric Antigen Receptor). International filing date April 29, 2016, earliest priority date April 30, 2015. Expiry date will be April 28, 2036 in most jurisdictions. Further patent term adjustments may apply in the US.
We are the exclusive licensee of a patent application owned by UCL Business plc covering a method of treatment using a T cell which expresses a Gamma Delta T cell receptor and a chimeric antigen receptor. The patent application claims are directed to GD-T cells expressing a co-stimulatory CAR, the advantages of the co-stimulatory CAR by inhibiting on-target, off-tumor activation due to its design, to the method and process of modifying a GD-T cell to express the co-stimulatory CAR, and to medical uses of the modified GD-T cell. National applications have been granted in Australia (AU 2016255611, expires April 28, 2036), allowed in Japan, and allowed in Israel (IL 255186) pending the statutory opposition period. Additional national applications are pending in:, Brazil, Canada, China, Hong Kong, South Korea, New Zealand, Singapore, South Africa, and the US. Regional applications are pending before the European and Eurasian Patent Offices.
WO 2016/005752 (Gamma Delta T cells and uses thereof). International filing date July 8, 2015, earliest priority date July 9, 2014. Expiry date for the patent granted in Israel will be July 7, 2035.
We own a patent application covering the method of preparing and using GD-T cells in the allogeneic treatment of subjects suffering from viral infection, fungal infection, protozoal infection or cancer. The patent application claims are directed to the process of providing GD-T cells from a first subject to a second subject (allogeneic transfer). Patent has been granted in Israel, national applications are pending in the US and Japan, and a regional application is pending before the European Patent Office
WO 2018/138522 (Immune cells with modified metabolism and their use thereof). International filing date January 26, 2018, earliest priority date January 26, 2017.
We own a patent application directed to gamma-delta T cells which overexpress the SLC1A5 amino acid transporter thereby improving tryptophan uptake in those cells and providing them with resistance to proliferative arrest in low tryptophan environments such as the tumour microenvironment. The patent also covers methods of engineering SLC1A5 overexpressing T cells. National applications are pending in: Australia, Brazil, Canada, China, Hong Kong, Israel, Japan, South Korea, New Zealand, Singapore, South Africa, and the US. Regional applications are pending before the European and Eurasian Patent Offices.
WO 2019/064030 (Modified CAR-T). International filing date October 1, 2018, earliest priority date September 29, 2017.
| 73 |
We own a patent application covering chimeric antigen receptors comprising an intracellular signaling domain derived from GD-T cell surface receptors. When expressed in GD or natural killer (NK) cells, the resultant CAR-T cells exhibit improved cytotoxicity. National applications are pending in: Australia, Brazil, Canada, China, Hong Kong, Israel, Japan, South Korea, New Zealand, Singapore, South Africa, and the US. Regional applications are pending before the European and Eurasian Patent Offices.
GB 2114059.5 CAR-Towed: Gamma Delta T cells modified with CARs without an endodomain. Filing date September 30, 2021.
We own a patent application covering chimeric antigen receptor constructs which lack a functional intracellular signaling domain and which are capable of binding to a target antigen which identifies a stressed or transformed cell. The constructs may be expressed in GD-T cells or natural killer (NK) cells. We anticipate that GB 2015543.8 will include composition of matter, methods of manufacture and method of use claims. A priority application has been filed in the UK.
GB 2104070.4 (Antigen binders and uses thereof). Filing date March 23, 2021
We own a patent application covering novel antibodies and antibody fragments capable of binding the B7H4 protein, to chimeric antigen receptors (CARs) incorporating a said antibody fragment, to T cells expressing the said CARs and to medical uses of those T cells. We anticipate that GB 2104070.4 will include composition of matter, methods of manufacture and method of use claims. A priority application has been filed in the UK.
GB 2569692 (T cell antigen receptor chimera). Filing date October 30, 2018.
In addition to the above 6 patent families and license for a patent family, we own a published patent application covering antigen receptor chimeras incorporating the antigen-binding specificity of an alpha-beta T cell receptor with a costimulatory only intracellular signaling domain, for example as discussed in the above pending patent applications derived from WO2016/166544. This application was allowed to publish in the UK, thereby establishing it as prior art against potential competitors, but was not progressed to examination.
Platform technology patent applications – We have several other patent applications in the process of being drafted, improving T cell efficacy by modulating PD1 expression, additional methods of expanding GD-T1 gamma-delta T cell populations and improvements to our GD CAR-T platform
Government Regulation and Product Approval
As a biopharmaceutical company, we are subject to extensive regulation. Our product candidates, if approved, will be regulated as biological medicines. With this classification, commercial production of our products will need to occur in registered and licensed facilities in compliance with current Good Manufacturing Practices, or cGMPs, for biologics.
Human immunotherapy products are a new category of therapeutics. The FDA categorizes human cell- or tissue-based products as either minimally manipulated or more than minimally manipulated and has determined that more than minimally manipulated products require clinical trials to demonstrate product safety and efficacy and the submission of a Biologics License Application, or BLA, for marketing authorization.
Government authorities in the United States (at the federal, state and local level) and in other countries and jurisdictions, including the European Union, extensively regulate, among other things, the research, development, preclinical and clinical testing, manufacturing, quality control, labeling, packaging, storage, record-keeping, promotion, advertising, sale, distribution, post-approval monitoring and reporting, marketing and export and import of biopharmaceutical products such as those we are developing. Our product candidates must be approved by the FDA before they may be legally marketed in the United States and by the appropriate foreign regulatory agency before they may be legally marketed in foreign countries. Generally, our activities in other countries will be subject to regulation that is similar in nature and scope as that imposed in the United States, although there can be important differences. Additionally, some significant aspects of regulation in Europe are addressed in a centralized way, but country-specific regulation remains essential in many respects. The process for obtaining regulatory marketing approvals and the subsequent compliance with applicable federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources.
| 74 |
United States Product Development Process
In the United States, the FDA regulates biological products under the Public Health Service Act, or PHSA, and the Federal Food, Drug and Cosmetic Act, or FDCA, and implementing regulations. Products are also subject to other federal, state and local statutes and regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or after approval, may subject an applicant to administrative or judicial sanctions. FDA sanctions could include, among other actions, refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters and similar public notice of alleged non-compliance with laws, product recalls or withdrawals from the market, product seizures, total or partial suspension of production or distribution, fines, refusals of government contracts, restitution, disgorgement of profits, or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us. The process required by the FDA before a biological product may be approved for marketing in the United States generally involves the following:
| ● | completion of preclinical laboratory tests and animal studies according to Good Laboratory Practices, or GLPs, and applicable requirements for the humane use of laboratory animals or other applicable regulations; | |
| ● | submission to the FDA of an Investigational New Drug Application, or IND, which must become effective before human clinical trials may begin; | |
| ● | performance of adequate and well-controlled human clinical trials according to the FDA’s regulations commonly referred to as Good Clinical Practices, or GCPs, and any additional requirements for the protection of human research subjects and their health information, to establish the safety and efficacy of the proposed biological product for its intended use; | |
| ● | preparation and submission to the FDA of a Biologics License Application, or BLA, for marketing approval that includes substantive evidence of safety, purity, and potency from results of nonclinical testing and clinical trials; | |
| ● | satisfactory completion of one or more FDA inspections of the manufacturing facility or facilities where the biological product is produced to assess compliance with cGMP to assure that the facilities, methods and controls used in product manufacture are adequate to preserve the biological product’s identity, strength, quality and purity and, if applicable, the FDA’s current Good Tissue Practices, or GTPs, for the use of human cellular and tissue products; | |
| ● | potential FDA audit of the nonclinical study and clinical trial sites that generated the data in support of the BLA; | |
| ● | payment of user fees for FDA review of the BLA; and | |
| ● | FDA acceptance, review and approval, or licensure, of the BLA, which might include review by an advisory committee, a panel typically consisting of independent clinicians and other experts who provide recommendations as to whether the application should be approved and under what conditions. |
Before testing any biological product candidate, including our product candidates, in humans, the product candidate must undergo rigorous the preclinical testing. Preclinical tests, also referred to as nonclinical studies, include laboratory evaluations as well as in vitro and animal studies to assess the potential safety and efficacy of the product candidate. After sufficient preclinical testing has been conducted, the conduct of the preclinical tests must comply with federal regulations and requirements including GLPs. The clinical trial sponsor must submit an IND to the FDA before clinical testing can begin in the United States. An IND must contain the results of the preclinical tests, manufacturing information, analytical data, any available clinical data or literature, a proposed clinical protocol, an investigator’s brochure, a sample informed consent form, and other materials. Clinical trial protocols detail, among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria, and the parameters to be used to monitor subject safety, including stopping rules that assure a clinical trial will be stopped if certain adverse events should occur. Each protocol and any amendments to the protocol must be submitted to the FDA as part of the IND. Some preclinical testing, such as toxicity studies, may continue even after the IND is submitted.
| 75 |
The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA raises concerns or questions regarding the proposed clinical trials or places the trial on a clinical hold within that 30-day time period. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. The FDA may also impose clinical holds on a biological product candidate at any time before or during clinical trials due to safety concerns or non-compliance. If the FDA imposes a clinical hold, trials may not recommence without FDA authorization and then only under terms authorized by the FDA. Accordingly, we cannot be sure that submission of an IND will result in the FDA allowing clinical trials to begin, or that, once begun, issues will not arise that suspend or terminate such trials.
Further, each clinical trial must be reviewed and approved by an independent institutional review board, or IRB, at or servicing each institution at which the clinical trial will be conducted. An IRB is charged with protecting the welfare and rights of trial participants and considers such items as whether the risks to individuals participating in the clinical trials are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the form and content of the informed consent that must be signed by each clinical trial subject or his or her legal representative and must monitor the clinical trial until completed. Clinical trials involving recombinant or synthetic nucleic acid molecules also must be reviewed by an institutional biosafety committee, or IBC, a local institutional committee that reviews and oversees basic and clinical research conducted at that institution. The IBC assesses the safety of the research and identifies any potential risk to public health or the environment.
Clinical trials involve the administration of the biological product candidate to healthy volunteers or patients under the supervision of qualified investigators, generally physicians not employed by or under the trial sponsor’s control. Clinical trials must be conducted and monitored in accordance with the FDA’s regulations comprising the GCP requirements, including the requirement that all research patients provide informed consent.
Human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
| ● | Phase 1. The biological product is initially introduced into healthy human subjects and tested for safety. In the case of some products for severe or life-threatening diseases, especially when the product may be too inherently toxic to ethically administer to healthy volunteers, the initial human testing is often conducted in patients with the target disease or condition. | |
| ● | Phase 2. The biological product is evaluated in a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance, optimal dosage and dosing schedule. | |
| ● | Phase 3. Clinical trials are undertaken to further evaluate dosage, clinical efficacy, potency, and safety in an expanded patient population, generally at geographically dispersed clinical trial sites. These clinical trials are intended to generate enough data to statistically evaluate the efficacy and safety of the product for approval, to establish the overall risk to benefit profile of the product and to provide an adequate basis for product labeling. |
Phase 1, Phase 2 and Phase 3 clinical trials may not be completed successfully within any specified period, if at all.
Post-approval clinical trials, sometimes referred to as Phase 4 clinical trials, may be conducted after initial marketing approval. These clinical trials are used to gain additional experience from the treatment of patients in the intended therapeutic indication, particularly for long-term safety follow-up.
During all phases of clinical development, regulatory agencies require extensive monitoring and auditing of all clinical activities, clinical data, and clinical trial investigators. Annual progress reports detailing the results of the clinical trials must be submitted to the FDA. Written IND safety reports must be promptly submitted to the FDA, and the investigators for serious and unexpected adverse events, any findings from other studies, tests in laboratory animals or in vitro testing that suggest a significant risk for human patients, or any clinically important increase in the rate of a serious suspected adverse reaction over that listed in the protocol or investigator brochure. The sponsor must submit an IND safety report within 15 calendar days after the sponsor determines that the information qualifies for reporting. The sponsor also must notify the FDA of any unexpected fatal or life-threatening suspected adverse reaction within seven calendar days after the sponsor’s initial receipt of the information. The FDA or the sponsor or its data safety monitoring board, an independent group of experts that evaluates study data for safety and makes recommendations concerning continuation, modification, or termination of clinical trials, may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research patients are being exposed to an unacceptable health risk, including risks inferred from other unrelated immunotherapy trials. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the biological product has been associated with unexpected serious harm to patients.
| 76 |
Because this is a relatively new and expanding area of novel therapeutic interventions, there can be no assurance as to the length of the trial period, the number of patients the FDA will require to be enrolled in the trials in order to establish the safety, efficacy, purity and potency of immunotherapy products, or that the data generated in these trials will be acceptable to the FDA to support marketing approval.
Concurrently with clinical trials, companies usually complete additional nonclinical studies and must also develop additional information about the physical characteristics of the biological product as well as finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. To help reduce the risk of the introduction of adventitious agents with use of biological products, the PHSA emphasizes the importance of manufacturing control for products whose attributes cannot be precisely defined. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, the sponsor must develop methods for testing the identity, strength, quality, potency and purity of the final biological product. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the biological product candidate does not undergo unacceptable deterioration over its shelf life.
United States Review and Approval Processes
After the completion of clinical trials of a biological product, FDA approval of a BLA must be obtained before commercial marketing of the biological product. The BLA must include results of product development, laboratory and animal studies, human trials, information on the manufacture and composition of the product, proposed labeling and other relevant information. The testing and approval processes require substantial time and effort and there can be no assurance that the FDA will accept the BLA for filing and, even if filed, that any approval will be granted on a timely basis, if at all as the FDA has significant discretion to approve or reject the BLA and to require additional preclinical or clinical studies.
Under the Prescription Drug User Fee Act, or PDUFA, as amended, each BLA must be accompanied by a significant user fee. The FDA adjusts the PDUFA user fees on an annual basis. PDUFA also imposes an annual program fee for approved biological products. Fee waivers or reductions are available in certain circumstances, including a waiver of the application fee for the first application filed by a small business. Additionally, no user fees are assessed on BLAs for products designated as orphan drugs, unless the product also includes a non-orphan indication.
Within 60 days following submission of the application, the FDA reviews a BLA submitted to determine if it is substantially complete before the agency accepts it for filing. The FDA may refuse to file any BLA that it deems incomplete or not properly reviewable at the time of submission and may request additional information. In this event, the BLA must be resubmitted with the additional information. The resubmitted application also is subject to review before the FDA accepts it for filing. Once the submission is accepted for filing, the FDA begins an in-depth substantive review of the BLA. The FDA reviews the BLA to determine, among other things, whether the proposed product is safe, potent, and/or effective for its intended use, and has an acceptable purity profile, and whether the product is being manufactured in accordance with cGMP to assure and preserve the product’s identity, safety, strength, quality, potency and purity. The FDA may refer applications for novel biological products or biological products that present difficult questions of safety or efficacy to an advisory committee, typically a panel that includes clinicians and other experts, for review, evaluation and a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions. During the biological product approval process, the FDA also will determine whether a Risk Evaluation and Mitigation Strategy, or REMS, is necessary to ensure that the benefits of the product outweigh its risks and to assure the safe use of the biological product, which could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. FDA determines the requirement for a REMS, as well as the specific REMS provisions, on a case-by-case basis. If the FDA concludes a REMS is needed, the sponsor of the BLA must submit a proposed REMS. The FDA will not approve a BLA without a REMS, if required.
| 77 |
Before approving a BLA, the FDA will inspect the facilities at which the product is manufactured. The FDA will not approve the product unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. For immunotherapy products, the FDA also will not approve the product if the manufacturer is not in compliance with the GTPs, to the extent applicable. These are FDA regulations and guidance documents that govern the methods used in, and the facilities and controls used for, the manufacture of human cells, tissues, and cellular and tissue based products, or HCT/Ps, which are human cells or tissue intended for implantation, transplant, infusion, or transfer into a human recipient. The primary intent of the GTP requirements is to ensure that cell and tissue based products are manufactured in a manner designed to prevent the introduction, transmission and spread of communicable disease. FDA GTP regulations also require tissue establishments to register and list their HCT/Ps with the FDA and, when applicable, to evaluate donors through screening and testing. Additionally, before approving a BLA, the FDA will typically inspect one or more clinical sites to assure that the clinical trials were conducted in compliance with IND trial requirements and GCP requirements.
To assure cGMP, GTP and GCP compliance, an applicant must incur significant expenditure of time, money and effort in the areas of training, recordkeeping, production, and quality control.
Notwithstanding the submission of relevant data and information, the FDA may ultimately decide that the BLA does not satisfy its regulatory criteria for approval and deny approval. If the agency decides not to approve the BLA in its then current form, the FDA will issue a Complete Response Letter, which generally outlines the specific deficiencies in the BLA identified by the FDA and may require additional clinical or other data or impose other conditions that must be met in order to secure final approval of the application. The deficiencies identified may be minor, for example, requiring labeling changes, or major, for example, requiring additional clinical trials. Even with the submission of additional information, the FDA may ultimately decide that the application does not satisfy the regulatory criteria for approval. If a Complete Response Letter is issued, the applicant may either resubmit the BLA, addressing all of the deficiencies identified in the letter, or withdraw the application.
If a product receives regulatory approval, the approval is limited to the conditions of use (e.g., patient population, indication) described in the application.
Further, the FDA may require that certain contraindications, warnings or precautions be included in the product labeling, or otherwise limit the scope of any approval. In addition, the FDA may require post marketing clinical trials, sometimes referred to as Phase 4 clinical trials, designed to further assess a biological product’s safety and effectiveness, and testing and surveillance programs to monitor the safety of approved products that have been commercialized. After approval, many types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further testing requirements and FDA review and approval.
In addition, under the Pediatric Research Equity Act, or PREA, a BLA or supplement to a BLA must contain data to assess the safety and effectiveness of the product for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may grant deferrals for submission of data or full or partial waivers.
United States Post-Approval Requirements
Any products for which we receive FDA approvals are subject to continuing regulation by the FDA, including, among other things, record-keeping requirements, reporting of adverse experiences with the product, providing the FDA with updated safety and efficacy information, product sampling and distribution requirements, and complying with FDA promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, restrictions on promoting products for uses or in patient populations that are not described in the product’s approved uses (known as “off-label use”), limitations on industry-sponsored scientific and educational activities, and requirements that important safety information and material facts related to the product be disclosed. Although physicians may prescribe legally available products for off-label uses, if the physicians deem to be appropriate in their professional medical judgment, manufacturers may not market or promote such off-label uses. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant civil, criminal and administrative liability.
| 78 |
In addition, quality control and manufacturing procedures must continue to conform to applicable manufacturing requirements after approval to ensure the long-term stability of the product. We currently are making clinical trial product in our own facilities in Scotland, United Kingdom. In the future, however, we expect to rely, on third parties for the production of commercial quantities of our products in accordance with cGMP regulations. cGMP regulations require among other things, quality control and quality assurance as well as the corresponding maintenance of records and documentation and the obligation to investigate and correct any deviations from cGMP. Manufacturers and other entities involved in the manufacture and distribution of approved products are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMP and other laws. Accordingly, manufacturers must continue to expend time, money, and effort in the area of production and quality control to maintain cGMP compliance. Discovery of problems with a product after approval may result in restrictions on a product, manufacturer, or holder of an approved BLA, including, among other things, recall or withdrawal of the product from the market.
The FDA also may require post-marketing testing, known as Phase 4 testing, and surveillance to monitor the effects of an approved product. Discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, with manufacturing processes, or the failure to comply with applicable FDA requirements can have negative consequences, including adverse publicity, judicial or administrative enforcement, complete withdrawal from the market, product recalls, warning letters from the FDA, mandated corrective advertising or communications with doctors, product seizure or detention, injunctions, and civil or criminal penalties, among others. Newly discovered or developed safety or effectiveness data may require changes to a product’s approved labeling, including the addition of new warnings and contraindications, and also may require the implementation of other risk management measures. Also, new government requirements, including those resulting from new legislation, may be established, or the FDA’s policies may change, which could delay or prevent regulatory approval of our products under development.
United States Marketing Exclusivity
The Biologics Price Competition and Innovation Act amended the PHSA to authorize the FDA to approve similar versions of innovative biologics, commonly known as biosimilars. Biosimilars are approved pursuant to an abbreviated pathway whereby applicants need not submit the full slate of preclinical and clinical data, and approval is based in part on the FDA’s findings of safety, purity, and potency for the original biologic (i.e., the reference product). Original BLAs are eligible to receive 12 years of exclusivity from the time of first licensure of the product, which prevents the FDA from approving any biosimilars to the reference product through the abbreviated pathway, but does not prevent approval of BLAs that are accompanied by a full data package and that do not rely on the reference product. A biosimilar may be approved if the product is highly similar to the reference product notwithstanding minor differences in clinically inactive components and there are no clinically meaningful differences with the reference product in terms of the safety, purity, and potency.
Pediatric exclusivity is another type of regulatory market exclusivity in the United States. Pediatric exclusivity, if granted, adds six months to existing exclusivity periods and patent terms. This six-month exclusivity, which runs from the end of other exclusivity protection or patent term, may be granted based on the voluntary completion of a pediatric trial in accordance with an FDA-issued “Written Request” for such a trial.
United States Coverage, Pricing and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any product candidates for which we obtain regulatory approval. In the United States and markets in other countries, sales of any products for which we receive regulatory approval for commercial sale will depend, in significant part, on the extent to which third-party payors provide coverage, and establish adequate reimbursement levels for such products. In the United States, third-party payers include federal and state healthcare programs, private managed care organizations, health insurers and other organizations. The process for determining whether a third-party payer will provide coverage for a product may be separate from the process of establishing the reimbursement rate that such a payor will pay for the product. Third-party payors may limit coverage to specific products on an approved list, also known as a formulary, which might not include all of the FDA-approved products for a particular indication. Third-party payors are increasingly challenging the price, examining the medical necessity of and reviewing the cost-effectiveness of medical products, therapies and services, in addition to questioning their safety and efficacy.
| 79 |
Reimbursement may impact the demand for, and/or the price of, any product candidate which obtains marketing approval. Even if coverage and reimbursement is obtained for a given product candidate by a third-party payor, the resulting reimbursement payment rates may not be adequate or may require co-payments that patients find unacceptably high. Patients who are prescribed medications for the treatment of their conditions, and their prescribing physicians, generally rely on third-party payors to reimburse all or part of the costs associated with those medications. Patients are unlikely to use a product, and physicians may be less likely to prescribe a product, unless coverage is provided and reimbursement is adequate to cover all or a significant portion of the cost of the product. Therefore, coverage and adequate reimbursement is critical to new drug product acceptance.
Different pricing and reimbursement schemes exist in other countries. In the EU, governments influence the price of pharmaceutical products through their pricing and reimbursement rules and control of national healthcare systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed. To obtain reimbursement or pricing approval, some of these countries may require the completion of additional clinical trials that compare the cost-effectiveness of a particular product candidate to currently available therapies. Other member states allow companies to fix their own prices for medicines, but monitor and control company profits. In addition, in some countries, cross-border imports from low-priced markets exert a commercial pressure on pricing within a country.
The downward pressure on healthcare costs in general, particularly prescription drugs and biologics, has become very intense. Governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. As a result, increasingly high barriers are being erected to the entry of new products. The marketability of any product candidates for which we receive regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide coverage and adequate reimbursement. In addition, emphasis on managed care in the United States has increased and we expect will continue to increase the pressure on healthcare pricing. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
United States Healthcare Laws Governing Interactions with Healthcare Providers
In addition to FDA restrictions on marketing of pharmaceutical products, several other types of state and federal laws restrict our business activities, including certain marketing practices. These laws include, without limitation, anti-kickback laws, false claims laws, data privacy and security laws, as well as transparency laws regarding payments or other items of value provided to healthcare providers.
The U.S. federal Anti-Kickback Statute prohibits any person or entity from, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item, good, facility or service reimbursable, in whole or in part, under Medicare, Medicaid or other federal healthcare programs. The term “remuneration” has been broadly interpreted to include anything of value. This statute has been interpreted to apply to arrangements between pharmaceutical manufacturers on the one hand and prescribers, purchasers and formulary managers on the other hand. Although there are a number of statutory exceptions and regulatory safe harbors protecting certain common activities from prosecution or other regulatory sanctions, the exceptions and safe harbors are drawn narrowly, and practices that involve remuneration that are alleged to be intended to induce prescribing, purchases or recommendations may be subject to scrutiny if they do not qualify for an exception or safe harbor. Failure to meet all of the requirements of a particular applicable statutory exception or regulatory safe harbor does not make the conduct per se illegal under the U.S. federal Anti-Kickback Statute. Instead, the legality of the arrangement will be evaluated on a case-by-case basis based on a cumulative review of all its facts and circumstances. Several courts have interpreted the statute’s intent requirement to mean that if any one purpose of an arrangement involving remuneration is to induce referrals of federal healthcare covered business, the U.S. federal Anti-Kickback Statute has been violated. Additionally, the intent standard under the U.S. federal Anti-Kickback Statute was amended by the Patient Protection and Affordable Care Act of 2010, as amended by the Health Care and Education Reconciliation Act of 2010, collectively the Affordable Care Act, or ACA, to a stricter standard such that a person or entity no longer needs to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. In addition, the ACA codified case law that a claim including items or services resulting from a violation of the U.S. federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the U.S. federal False Claims Act.
| 80 |
Federal civil and criminal false claims laws and civil monetary penalties laws, including the U.S. federal False Claims Act, which can be enforced through civil whistleblower or qui tam actions, prohibit any person or entity from, among other things, knowingly presenting, or causing to be presented, a false claim for payment to the federal government, or knowingly making, or causing to be made, a false statement to have a false claim paid. Pharmaceutical and other healthcare companies have been prosecuted under these laws for, among other things, allegedly inflating drug prices they report to pricing services, which in turn were used by the government to set Medicare and Medicaid reimbursement rates, and for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. In addition, certain marketing practices, including off-label promotion, may also violate false claims laws. Further, pharmaceutical manufacturers can be held liable under the U.S. federal False Claims Act even when they do not submit claims directly to government payors if they are deemed to “cause” the submission of false or fraudulent claims.
The U.S. federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, created new federal criminal statutes that prohibit among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third- party payors, knowingly and willfully embezzling or stealing from a healthcare benefit program, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Like the U.S. federal Anti-Kickback Statute, the ACA amended the intent standard for certain healthcare fraud under HIPAA such that a person or entity no longer needs to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH, and their implementing regulations, impose certain requirements on “covered entities,” including certain healthcare providers, health plans and healthcare clearinghouses, as well as their respective “business associates” that create, receive, maintain or transmit individually identifiable health information for or on behalf of a covered entity, and their covered subcontractors, relating to the privacy, security, transmission and breach of individually identifiable health information. Further, HITECH also created four new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates, and gave state attorneys general new authority to file civil actions for damages or injunctions in U.S. federal courts to enforce HIPAA and seek attorneys’ fees and costs associated with pursuing federal civil actions.
Additionally, the federal Physician Payments Sunshine Act, created under the ACA, and its implementing regulations, require certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to annually report to the Centers for Medicare and Medicaid Services, or CMS, information related to certain payments or other transfers of value provided to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, or to entities or individuals at the request of, or designated on behalf of, the physicians and teaching hospitals as well as certain ownership and investment interests held by physicians and their immediate family members. Beginning in 2022, applicable manufacturers also will be required to report information regarding payments and transfers of value provided to physician assistants, nurse practitioners, clinical nurse specialists, certified nurse anesthetists, anesthesiologist assistants, and certified nurse-midwives.
Additionally, similar healthcare laws and regulations in the European Union and other jurisdictions, including reporting requirements detailing interactions with and payments to healthcare providers and laws governing the privacy and security of certain protected information, such as GDPR, which imposes obligations and restrictions on the collection and use of personal data relating to individuals located in the European Union (including health data).
| 81 |
Finally, the majority of states also have statutes or regulations similar to the aforementioned federal laws, some of which are broader in scope and apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor. Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government in addition to requiring drug manufacturers to report information related to payments to clinicians and other healthcare providers or marketing expenditures. Some states and local jurisdictions require the registration of pharmaceutical sales representatives. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Because of the breadth of these laws and the narrowness of their exceptions and safe harbors, it is possible that business activities can be subject to challenge under one or more of such laws. The scope and enforcement of each of these laws is uncertain and subject to rapid change in the current environment of healthcare reform, especially in light of the lack of applicable precedent and regulations. Federal and state enforcement bodies have recently increased their scrutiny of interactions between healthcare companies and healthcare providers, which has led to a number of investigations, prosecutions, convictions and settlements in the healthcare industry.
Ensuring that business arrangements with third parties comply with applicable healthcare laws and regulations is costly and time consuming. If business operations are found to be in violation of any of the laws described above or any other applicable governmental regulations a pharmaceutical manufacturer may be subject to penalties, including civil, criminal and administrative penalties, damages, fines, disgorgement, individual imprisonment, exclusion from governmental funded healthcare programs, such as Medicare and Medicaid, contractual damages, reputational harm, diminished profits and future earnings, additional reporting obligations and oversight if subject to a corporate integrity agreement or other agreement to resolve allegations of non-compliance with these laws, and curtailment or restructuring of operations, any of which could adversely affect a pharmaceutical manufacturer’s ability to operate its business and the results of its operations.
United States Healthcare Reform Efforts
A primary trend in the United States healthcare industry and elsewhere is cost containment. Over the last several years, there have been federal and state proposals and legislation enacted regarding the pricing of pharmaceutical and biopharmaceutical products, limiting coverage and reimbursement for drugs and other medical products, and making changes to healthcare financing and the delivery of care in the United States.
There continues to be heightened Congressional scrutiny in the United States of pharmaceutical pricing practices designed to, among other things, bring more transparency in product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for products. At the state level, legislatures have increasingly enacted legislation and implemented regulations designed to control pharmaceutical and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. In addition, regional healthcare authorities and individual hospitals are increasingly using bidding procedures to determine what pharmaceutical products and which suppliers will be included in their prescription drug and other healthcare programs.
In addition, other federal health reform measures have been proposed and adopted in the United States that could impact cell therapy. Most notably, there has been political support for rules related to value-based payment alternatives in the Medicaid program. Medicaid is a jointly run federal and state program that provides health benefits coverage for low-income residents and children. In exchange for broad coverage in Medicaid, drug manufacturers are required to sign a Medicare Drug Rebate agreement which requires them to offer Medicaid programs the “best price” available for a particular product. This “best price” takes into consideration any rebates or concessions manufacturers offer, with some exceptions. The final rule would exempt value-based or outcomes-based payment arrangements from the definition of “best price” which provides manufacturers more flexibility to work with commercial payers and states on innovate payment mechanisms for high-cost cell and gene therapies. While Medicaid is not a significant driver of cell therapy sales it is a bellwether program and one we watch closely.
| 82 |
United States FCPA, the Bribery Act and Other Laws
The FCPA, prohibits any U.S. individual or business from paying, offering, or authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate for the purpose of influencing any act or decision of the foreign entity in order to assist the individual or business in obtaining or retaining business. The FCPA also obligates companies whose securities are listed in the United States to comply with accounting provisions requiring the company to maintain books and records that accurately and fairly reflect all transactions of the corporation, including international subsidiaries, and to devise and maintain an adequate system of internal accounting controls for international operations. Activities that violate the FCPA, even if they occur wholly outside the United States, can result in criminal and civil fines, imprisonment, disgorgement, oversight, and debarment from government contracts.
Our operations are also subject to non-U.S. anti-corruption laws such as the Bribery Act. As with the FCPA, these laws generally prohibit us and our employees and intermediaries from authorizing, promising, offering, or providing, directly or indirectly, improper or prohibited payments, or anything else of value, to government officials or other persons to obtain or retain business or gain some other business advantage. Under the Bribery Act, we may also be liable for failing to prevent a person associated with us from committing a bribery offense.
We are also subject to other laws and regulations governing our international operations, including regulations administered by the governments of the United Kingdom and the United States and authorities in the European Union, including applicable export control regulations, economic sanctions and embargoes on certain countries and persons, anti-money laundering laws, import and customs requirements and currency exchange regulations, collectively referred to as trade control laws.
Failure to comply with the Bribery Act, the FCPA and other anti-corruption laws and trade control laws could subject us to criminal and civil penalties, disgorgement and other sanctions and remedial measures, and legal expenses.
Review and Approval of New Drug Products in the European Union
In the European Union, medicinal products, including advanced therapy medicinal products, or ATMPs, are subject to extensive pre- and post-market regulation by regulatory authorities at both the European Union and national levels. ATMPs comprise gene therapy products, somatic-cell therapy products and tissue engineered products, which are cells or tissues that have undergone substantial manipulation and that are administered to human beings in order to regenerate, repair or replace a human tissue. We anticipate that our therapy products will be regulated as ATMPs in the European Union. There is legislation at a European Union level relating to the standards of quality and safety for the collection and testing of human blood and blood components for use in cell-based therapies, which could apply to our products. Additionally, there may be local legislation in various European Union Member States, which may be more restrictive than the European Union legislation, and we would need to comply with such legislation to the extent it applies.
EU Clinical Trials
Clinical trials of medicinal products in the European Union must be conducted in accordance with European Union and national regulations and the International Conference on Harmonization, or ICH, guidelines on Good Clinical Practices, or GCP. Additional GCP guidelines from the European Commission, focusing in particular on traceability, apply to clinical trials of ATMPs. The sponsor must take out a clinical trial insurance policy, and in most European Union countries, the sponsor is liable to provide “no fault” compensation to any study subject injured in the clinical trial.
Prior to commencing a clinical trial, the sponsor must obtain a clinical trial authorization from the competent authority, and a positive opinion from an independent ethics committee. The application for a clinical trial authorization must include, among other things, a copy of the trial protocol and an investigational medicinal product dossier containing information about the manufacture and quality of the medicinal product under investigation. Currently, clinical trial authorization applications must be submitted to the competent authority in each EU Member State in which the trial will be conducted. Under the new Regulation on Clinical Trials, which is to take effect in December 2021, there will be a centralized application procedure where one national authority takes the lead in reviewing the application and the other national authorities have only a limited involvement. Any substantial changes to the trial protocol or other information submitted with the clinical trial applications must be notified to or approved by the relevant competent authorities and ethics committees. Medicines used in clinical trials must be manufactured in accordance with cGMP. Other national and European Union-wide regulatory requirements also apply.
| 83 |
During the development of a medicinal product, the EMA and national medicines regulators within the European Union provide the opportunity for dialogue and guidance on the development program. At the EMA level, this is usually done in the form of scientific advice, which is given by the Scientific Advice Working Party of the Committee for Medicinal Products for Human Use, or CHMP. A fee is incurred with each scientific advice procedure. Advice from the EMA is typically provided based on questions concerning, for example, quality (chemistry, manufacturing and controls testing), nonclinical testing and clinical studies, and pharmacovigilance plans and risk-management programs. In accordance with the EMA’s policy, scientific advice will not be legally binding with regard to any future marketing authorization application of the product concerned.
EU Marketing Authorizations
In order to market a new medicinal product in the European Union, a company must submit and obtain approval from regulators of a marketing authorization application, or MAA. The process for doing this depends, among other things, on the nature of the medicinal product.
The centralized procedure results in a single marketing authorization, or MA, granted by the European Commission that is valid across the EEA (i.e., the European Union as well as Iceland, Liechtenstein and Norway). The centralized procedure is compulsory for human drugs that are: (i) derived from biotechnology processes, such as genetic engineering, (ii) contain a new active substance indicated for the treatment of certain diseases, such as HIV/AIDS, cancer, diabetes, neurodegenerative diseases, autoimmune and other immune dysfunctions and viral diseases, (iii) officially designated orphan medicines and (iv) advanced-therapy medicines, such as gene therapy, somatic cell therapy or tissue-engineered medicines. The centralized procedure may at the request of the applicant also be used in certain other cases. Therefore, the centralized procedure would be mandatory for the products we are developing.
The Committee for Advanced Therapies, or CAT, is responsible in conjunction with the CHMP for the evaluation of ATMPs. The CAT is primarily responsible for the scientific evaluation of ATMPs and prepares a draft opinion on the quality, safety and efficacy of each ATMP for which a marketing authorization application is submitted. The CAT’s opinion is then taken into account by the CHMP when giving its final recommendation regarding the authorization of a product in view of the balance of benefits and risks identified. Although the CAT’s draft opinion is submitted to the CHMP for final approval, the CHMP may depart from the draft opinion, if it provides detailed scientific justification. The CHMP and CAT are also responsible for providing guidelines on ATMPs and have published numerous guidelines, including specific guidelines on gene therapies and cell therapies. These guidelines provide additional guidance on the factors that the EMA will consider in relation to the development and evaluation of ATMPs and include, among other things, the preclinical studies required to characterize ATMPs; the manufacturing and control information that should be submitted in a marketing authorization application; and post-approval measures required to monitor patients and evaluate the long-term efficacy and potential adverse reactions of ATMPs. Although these guidelines are not legally binding, we believe that our compliance with them is likely necessary to gain and maintain approval for any of our product candidates.
Under the centralized procedure in the European Union, the maximum timeframe for the evaluation of an MAA by the EMA is 210 days. This excludes so-called clock stops, during which additional written or oral information is to be provided by the applicant in response to questions asked by the CHMP. At the end of the review period, the CHMP provides an opinion to the European Commission. If this is opinion favorable, the Commission may then adopt a decision to grant an MA. In exceptional cases, the CHMP might perform an accelerated review of an MAA in no more than 150 days. This is usually when the product is of major interest from the point of view of public health and, in particular, from the viewpoint of therapeutic innovation.
| 84 |
The European Commission may grant a so-called “marketing authorization under exceptional circumstances”. Such authorization is intended for products for which the applicant can demonstrate that it is unable to provide comprehensive data on the efficacy and safety under normal conditions of use, because the indications for which the product in question is intended are encountered so rarely that the applicant cannot reasonably be expected to provide comprehensive evidence, or in the present state of scientific knowledge, comprehensive information cannot be provided, or it would be contrary to generally accepted principles of medical ethics to collect such information. Consequently, marketing authorization under exceptional circumstances may be granted subject to certain specific obligations, which may include the following:
| ● | the applicant must complete an identified program of studies within a time period specified by the competent authority, the results of which form the basis of a reassessment of the benefit/risk profile; | |
| ● | the medicinal product in question may be supplied on medical prescription only and may in certain cases be administered only under strict medical supervision, possibly in a hospital and in the case of a radiopharmaceutical, by an authorized person; and | |
| ● | the package leaflet and any medical information must draw the attention of the medical practitioner to the fact that the particulars available concerning the medicinal product in question are as yet inadequate in certain specified respects. |
A marketing authorization under exceptional circumstances is subject to annual review to reassess the risk-benefit balance in an annual reassessment procedure. Continuation of the authorization is linked to the annual reassessment and a negative assessment could potentially result in the marketing authorization being suspended or revoked. The renewal of a marketing authorization of a medicinal product under exceptional circumstances, however, follows the same rules as a “normal” marketing authorization. Thus, a marketing authorization under exceptional circumstances is granted for an initial five years, after which the authorization will become valid indefinitely, unless the EMA decides that safety grounds merit one additional five-year renewal.
The European Commission may also grant a so-called “conditional marketing authorization” prior to obtaining the comprehensive clinical data required for an application for a full marketing authorization. Such conditional marketing authorizations may be granted for product candidates (including medicines designated as orphan medicinal products), if (i) the risk-benefit balance of the product candidate is positive, (ii) it is likely that the applicant will be in a position to provide the required comprehensive clinical trial data, (iii) the product fulfills an unmet medical need and (iv) the benefit to public health of the immediate availability on the market of the medicinal product concerned outweighs the risk inherent in the fact that additional data are still required. A conditional marketing authorization may contain specific obligations to be fulfilled by the marketing authorization holder, including obligations with respect to the completion of ongoing or new studies, and with respect to the collection of pharmacovigilance data. Conditional marketing authorizations are valid for one year, and may be renewed annually, if the risk-benefit balance remains positive, and after an assessment of the need for additional or modified conditions and/or specific obligations. The timelines for the centralized procedure described above also apply with respect to the review by the CHMP of applications for a conditional marketing authorization.
EU Data Exclusivity
Marketing authorization applications for generic medicinal products do not need to include the results of preclinical and clinical trials, but instead can refer to the data included in the marketing authorization of a reference product for which regulatory data exclusivity has expired. If a marketing authorization is granted for a medicinal product containing a new active substance, that product benefits from eight years of data exclusivity, during which generic marketing authorization applications referring to the data of that product may not be accepted by the regulatory authorities, and a further two years of market exclusivity, during which such generic products may not be placed on the market. The two-year period may be extended to three years if during the first eight years a new therapeutic indication with significant clinical benefit over existing therapies is approved.
| 85 |
There is a special regime for biosimilars, or biological medicinal products that are similar to a reference medicinal product but that do not meet the definition of a generic medicinal product, for example, because of differences in raw materials or manufacturing processes. For such products, the results of appropriate preclinical or clinical trials must be provided, and guidelines from the EMA detail the type of quantity of supplementary data to be provided for different types of biological product. There are no such guidelines for complex biological products, such as gene or cell therapy medicinal products, and so it is unlikely that biosimilars of those products will currently be approved in the European Union. However, guidance from the EMA states that they will be considered in the future in light of the scientific knowledge and regulatory experience gained at the time.
EU Pediatric Development
In the European Union, companies developing a new medicinal product must agree to a Pediatric Investigation Plan, or PIP, with the EMA and must conduct pediatric clinical trials in accordance with that PIP, unless a deferral or waiver applies, (e.g., because the relevant disease or condition occurs only in adults). The marketing authorization application for the product must include the results of pediatric clinical trials conducted in accordance with the PIP, unless a waiver applies, or a deferral has been granted, in which case the pediatric clinical trials must be completed at a later date. Products that are granted a marketing authorization on the basis of the pediatric clinical trials conducted in accordance with the PIP are eligible for a six-month extension of the protection under a supplementary protection certificate (if any is in effect at the time of approval) or, in the case of orphan medicinal products, a two-year extension of the orphan market exclusivity. This pediatric reward is subject to specific conditions and is not automatically available when data in compliance with the PIP are developed and submitted.
EU Post-Approval Controls
The holder of a marketing authorization must establish and maintain a pharmacovigilance system and appoint an individual qualified person for pharmacovigilance, or QPPV, who is responsible for oversight of that system. Key obligations include expedited reporting of suspected serious adverse reactions and submission of periodic safety update reports, or PSURs.
All new marketing authorization applications must include a risk management plan, or RMP, describing the risk management system that the company will put in place and documenting measures to prevent or minimize the risks associated with the product. The regulatory authorities may also impose specific obligations as a condition of the marketing authorization. Such risk-minimization measures or post-authorization obligations may include additional safety monitoring, more frequent submission of PSURs, or the conduct of additional clinical trials or post-authorization safety studies. RMPs and PSURs are routinely available to third parties requesting access, subject to limited redactions. All advertising and promotional activities for the product must be consistent with the approved summary of product characteristics, and therefore all off-label promotion is prohibited. Direct-to-consumer advertising of prescription medicines is also prohibited in the European Union. Although general requirements for advertising and promotion of medicinal products are established under EU directives, the details are governed by regulations in each EU Member State and can differ from one country to another.
EU Pricing and Reimbursement in the European Union
Governments influence the price of medicinal products in the European Union through their pricing and reimbursement rules and control of national healthcare systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed. To obtain reimbursement or pricing approval, some of these countries may require the completion of clinical trials that compare the cost-effectiveness of a particular product candidate to currently available therapies. Other EU Member States allow companies to fix their own prices for medicines, but monitor and control company profits. The downward pressure on healthcare costs in general, particularly prescription medicines, has become very intense. As a result, increasingly high barriers are being erected to the entry of new products.
Brexit and the Regulatory Framework in the United Kingdom
The United Kingdom officially withdrew from the European Union on January 31, 2020 (“Brexit”). Pursuant to the formal withdrawal arrangements agreed between the United Kingdom and the European Union, the United Kingdom was subject to a transition period until December 31, 2020, or the Transition Period, during which European Union rules continued to apply. A trade and cooperation agreement, or the Trade and Cooperation Agreement, that outlines the future trading relationship between the United Kingdom and the European Union was agreed in December 2020.
| 86 |
Brexit may influence the attractiveness of the United Kingdom as a place to conduct clinical trials. The European Union’s regulatory environment for clinical trials is being harmonized as part of the Clinical Trial Regulations, which come into full effect at the end of 2021, but it is currently unclear as to what extent the United Kingdom will seek to align its regulations with the European Union. Failure of the United Kingdom to closely align its regulations with the EU may have an effect on the cost of conducting clinical trials in the United Kingdom as opposed to other countries and/or make it harder to seek a marketing authorization for our product candidates on the basis of clinical trials conducted in the United Kingdom.
In the short term there will be few changes to clinical trials that only have sites in the United Kingdom. The MHRA have confirmed that the sponsor of a clinical trial can be based in the EEA for an initial period following Brexit. Further investigational medicinal products can be supplied directly from the EU/EEA to a trial site in the United Kingdom without further oversight until January 1, 2022, and to Northern Ireland beyond such date. The United Kingdom is now a “third country” for the purpose of clinical trials that have sites in the EEA. For such trials the sponsor/legal representative must be based in the EEA, and the trial must be registered on the EU Clinical Trials Register (including data on sites outside of the EEA).
The data exclusivity periods in the United Kingdom are currently in line with those in the European Union, but the Trade and Cooperation Agreement provides that the periods for both data and market exclusivity are to be determined by domestic law, and so there could be divergence in the future. It is currently unclear whether the MHRA in the United Kingdom is sufficiently prepared to handle the increased volume of marketing authorization applications that it is likely to receive.
Orphan designation in the United Kingdom following Brexit is based on the prevalence of the condition in the United Kingdom as opposed to the current position where prevalence in the European Union is the determinant. It is therefore possible that conditions that are currently designated as orphan conditions in the United Kingdom will no longer be and that conditions that are not currently designated as orphan conditions in the European Union will be designated as such in the United Kingdom.
EU Orphan Drug Designation
The European Medicines Agency (EMA) and FDA play a central role in facilitating the development and authorization of medicines for rare diseases, which are termed ‘orphan medicines’ in the medical world. In the EU, sponsors who obtain orphan designation benefit from protocol assistance, a type of scientific advice specific for designated orphan medicines, and market exclusivity once the medicine is on the market. Fee reductions are also available depending on the status of the sponsor and the type of service required. When planning the development of their medicinal product, sponsors should consult the relevant scientific guidelines.
The general therapeutic strategy for the treatment of AML has not changed substantially over the past 30 years. Excluding APL (which should be treated with all trans-retinoic acid), AML management is based primarily on induction, incorporating an anthracycline and cytarabine, and consolidation therapy, and/or allogeneic Hematopoietic Stem Cell Transplantation (alloHSCT). Induction/consolidation therapy leads to high CRs rates in those who are eligible for treatment and present a favourable risk profile.
Several novel agents are in various stages of development for the treatment of AML. Novel approaches include antibody-based immunotherapy and adoptive cell therapy that aim to improve anti-leukaemia T cell function, such as the therapies developed by TCB (OmnImmune®). OmnImmune® (TCB002) was initially studied in patients with active relapsed or refractory AML who are not eligible or do not consent to high dose salvage chemotherapy and/or alloHSCT. In July 2019, OmnImmune® (TCB002) was granted ‘orphan medicine’ status from the FDA for Acute Myeloid Leukaemia (AML). As a follow on to OmnImmune® (TCB002), TCB intends to conduct phase 2b/3 studies to treat earlier stage AML and expects to commence treating patients in these trials (as OmnImmune® (TCB008-001)) in H1 2022.
| 87 |
Legal Proceedings
From time to time, we may be party to litigation that arises in the ordinary course of our business. We do not have any pending litigation that, separately or in the aggregate, would, in the opinion of management, have a material adverse effect on our results of operations, financial condition or cash flows.
| C. | Organizational Structure |
Currently, we have three, wholly owned, subsidiaries, (i) TC BioPharm Limited, incorporated on July 1, 2013, through which we to conduct our principal operations, and (ii) two subsidiaries (a) TC BioPharm BV, incorporated in The Netherlands in March 2019 and (b) TC BioPharm (North America) Inc., incorporated in the United States of America in June 2021, that currently have minimal operations. It is anticipated that TC BioPharm (North America) Inc. will develop operations and a management presence in the United States, with a view to expanding our product offerings into that jurisdiction in the future.
| D. | Property Plant and Equipment |
Our corporate headquarters and most of our operations, including our research and manufacturing facilities, are located at Maxim 1, 2 Parklands Way, Holytown, Motherwell, ML1 4WR, United Kingdom. The lease for this space expires February 28, 2029 and covers a total leasable area of approximately 26,300 square feet. We believe that our office facilities and the production and research facilities in the United Kingdom are sufficient to meet our current needs.
| Item 4A. | Unresolved Staff Comments |
Not applicable.
| Item 5. | Operating and Financial Review and Prospects |
Our actual results may differ materially from those contained in or implied by any forward-looking statements.
| A. | Operating Results |
You should read the following discussion and analysis of financial condition and operating results together with the information in our consolidated financial statements and the related notes to those statements included elsewhere in this Annual Report. We present our consolidated financial statements in pounds sterling and in accordance with International Financial Reporting Standards, or IFRS, as issued by the International Accounting Standards Board, or IASB, which may differ in material respects from generally accepted accounting principles in other jurisdictions, including generally accepted accounting principles in the United States, or U.S. GAAP.
The statements in this discussion regarding industry outlook, our expectations regarding our future performance, liquidity and capital resources and other non-historical statements are forward-looking statements. These forward-looking statements are subject to numerous risks and uncertainties, including the risks and uncertainties described in the sections titled “Risk Factors.” Our actual results may differ materially from those contained in the following discussion and analysis, as well as the section titled “Special Note Regarding Forward-Looking Statements.”
| 88 |
Our books and records are maintained in pounds sterling. For the purposes of convenience to the reader, we have translated pound sterling amounts as of and for the year ended December 31, 2021 into US Dollars at the rate of £1.00 to $1.3500, which was the noon buying rate of the Federal Reserve Bank of New York on December 30, 2021. These translations should not be considered representations that any such amounts have been, could have been, or could be converted into US Dollars at that or any other exchange rate as of that date or any other date.
TC BioPharm (Holdings) plc was incorporated on October 25, 2021. On December 17, 2021, all shareholders in TC BioPharm Limited and holders of convertible loan notes in TC BioPharm Limited exchanged their shares and convertible loan notes for the same number and classes of newly issued shares and/or convertible loan notes in TC BioPharm (Holdings) plc and, as a result, TC BioPharm Limited became a wholly owned subsidiary of TC BioPharm (Holdings) plc. The corporate reorganization has been accounted for as a business combination under common control and therefore, TC BioPharm (Holdings) plc is a continuation of TC BioPharm Limited and its subsidiaries. The corporate reorganization has been given retrospective effect in these consolidated financial statements, which represent the consolidated financial statements of TC BioPharm (Holdings) plc. All TC BioPharm Limited share options granted to directors and employees under share option plans that were in existence immediately prior to the reorganization were exchanged for share options in TC BioPharm (Holdings) plc on a one-for-one basis with no change in any of the terms or conditions.
On December 17, 2021 and subsequent to the group reorganization, the Company undertook a share split such that one issued share was exchanged for ten new shares. As a result of the forward share split, all references in the Operating and Financial review to units of ordinary shares or per share amounts are reflective of the forward share split for all periods presented. In addition, the exercise prices and the numbers of shares issuable upon the exercise of any outstanding options to purchase ordinary shares were proportionally adjusted pursuant to the respective anti-dilution terms of the share-based payment plans.
On February 10, 2022, TC BioPharm (Holdings) plc completed an initial public offering on the Nasdaq Capital Market and since then, our ADSs and public warrants have been listed under the symbols TCBP and TCBPW, respectively.
Overview
TC BioPharm (Holdings) plc (TCB) is a clinical-stage biopharmaceutical company with a cell-based product pipeline capable of treating a variety of disorders including cancer and infectious disease.
TCB is currently developing a pipeline of unmodified allogeneic GD-T therapies and next generation GD CAR-T treatments with a number of advantages over conventional approaches. TC BioPharm owns its two main patent families in the GD CAR-T space, providing robust IP protection and manufactures all products in-house, leading to a much lower cost of goods than competitor products.
Conventional CAR-T treatments have seen many patients experience treatment-related adverse events and are limited to liquid tumors. Furthermore, the cost of manufacture of such treatments is high which can lead to difficulties in scaling an infrastructure to meet patient demand.
Our approach takes advantage of the inherent specificity of GD-T cells against phosphoantigens which are expressed only by cancerous and infected cells. This ensures that the cytotoxic effect of the CAR-expressing GD-T cells will be focused on the pathogenic cells expressing the target antigen whilst ignoring healthy cells. This is ensured by the fact that when the target antigen is expressed on a healthy cell, the GD CAR-T cell is not activated. This technology enables the targeting of cell surface antigens which have previously been deemed ‘undruggable’ due to their expression on healthy/non-diseased tissue. Thus, our CAR-T products have the potential to treat a wider range of tumors than can be targeted with present strategies.
| 89 |
Going concern
The Company was incorporated in 2014 to develop therapeutic products based around its gamma delta T cell platform technology, with the objective of conducting clinical trials to demonstrate safety and efficacy and eventually being granted regulatory approval to market and sell its products. This activity was expected to be ongoing over several years and has involved considerable expenditure to date on carrying out research and development and conducting clinical trials. In common with most development and/or clinical stage biotechnology companies, the Company has not yet generated any revenues from sales of products, but has obtained cash to finance its research, development and clinical trial activities from equity, debt and grant financings and from receipts from partners under collaborative co-development agreements. The Company is expected to stay in this clinical development stage for several years before any product becomes marketable. The Company therefore expects to continue to incur significant losses in the foreseeable future.
As at December 31, 2021, the Company had an accumulated deficit of £33.5 million. It experienced negative cash flows from operating activities during the year ended December 31, 2021, of £5.3 million, and expects to incur continued negative cash flows for the foreseeable future. Net losses incurred for the year ended December 30, 2021, and 2020, amounted to £13.6 million and £5.5 million, respectively.
As at December 31, 2021, the Company’s cash and cash equivalents amounted to £1.6 million, current assets amounted to £3.9 million and current liabilities (excluding amounts which may become payable under its Convertible Loan Notes, referred to further below) amounted to £6.8 million.
In February 2022 the Company raised $17.5million (£13.0 million) ($14.5m (£10.7 million) net of all commissions, costs and expenses) through the completion of an initial public offering of its ADS and Warrants on Nasdaq (IPO).
The Company received $8.8 million (£6.5 million) in cash in the year ended December 31, 2021, through the issuance of Convertible Loan Notes (‘Notes’). The Notes were issued in United States dollars at a 50% discount to their face value (i.e., for every $2 of face value of note issued the Company received $1). Thus, we have issued a total of $17.7 million (£13.1 million) of Loans at face value (in exchange for aggregate cash receipts of $8.8 million). Of this face value amount, $13.1 million was converted, in accordance with the terms of the Notes, into ADSs and Warrants at the IPO Date, leaving $4.6 million (£3.4 million) face value of the Notes outstanding at the date hereof. Unless otherwise agreed between the Company and the individual Note holders the outstanding Notes will convert into ADSs and Warrants (at a conversion price of 1 ADS and 2 Warrants per $4.25 of the face value of the converted Notes, plus 5% interest accruing) in May and August 2022, and, if not converted or renegotiated, they will become repayable at their face value (plus 5% interest accruing). With respect to the Notes redeemable in May 2022, the Noteholders have elected to be repaid. The amount that is repayable in May 2022 under the terms of the Notes, is $2.4 million (£1.8 million). The balance of the outstanding face value ($2.2 million (£1.6 million) plus interest), if not renegotiated or converted, becomes repayable in August 2022.
On April 30, 2022, the Company had cash on hand of $12.7 million (£9.4 million), which will not be sufficient to enable the Company to meet the cash requirements required to enable it to conduct its business plan through the going concern period (being to May 31, 2023) (“Going Concern Period”). With existing resources, we expect to be able to fund operations into Q4 2022, or early Q3 2022 if our Convertible Loan Note holders opt for repayment
In common with many early-stage biotechnology companies our future liquidity needs, and ability to address them, will largely be determined by the availability of capital, both generally and in particular to fund our product candidates and key development and regulatory projects. We anticipate having to raise capital routinely on the capital markets, taking advantage of our public listing. We are currently progressing various cash accretive initiatives to fill the gap in short-term working capital referred to above, which could be in the form of an equity raise or other forms of financings such as collaborations or licensing arrangements.
| 90 |
We believe that these initiatives should improve our net short-term working capital position sufficiently to provide sufficient capital to finance planned operations into early 2023, and, before then, we would expect to be in a position to raise significantly greater capital to fund our longer-term plan. However, there can be no certainty that these initiatives will be successful and, if they are not, management will seek to deploy alternative plans, which could have a potentially significant negative impact on shareholder and asset value. Such plans could include all or any of the following: raising additional capital through low priced and/or complex equity and/or debt financings; entering transactions involving sales, joint venturing or licensing of intellectual property; reducing and/or deferring discretionary spending on research and development or clinical programs; restructuring our operating model to take advantage of our manufacturing capability to generate short term revenues; reducing our cash burn rate through reduction in planned operating costs. The accompanying consolidated financial statements have been prepared in conformity with IFRS as issued by IASB, which contemplate continuation of the Company as a going concern (having adequate working capital to maintain operations through the Going Concern Period). The Company has not established a source of revenues sufficient to cover its operating costs, and as such, has been dependent on funding operations primarily through the sale of securities, commercial partnerships, and/or grants. The Company expects to incur further losses over the next several years as it develops its clinical products towards the market. The Company has spent, and expects to continue to spend, substantial amounts of funding to implement its business strategy. Although the completion of its IPO on Nasdaq was a major milestone for the Company, as it opens much wider avenues to raise future finance, the market conditions were such that the offering raised less than was initially targeted, and the proceeds of the offering alone are not adequate to finance the Company’s clinical and product development programs through the Going Concern Period. Nonetheless the proceeds of the offering, together with the anticipated proceeds from various initiatives referred to above, cause management to believe that the Company will have sufficient liquidity to fund its operations through the Going Concern Period, and, on that basis management continues to view the Company as a going concern.
Notwithstanding this, management recognizes that there is considerable risk in both (i) the ability of the Company to implement successfully the short term working capital that it requires to maintain operations through the Going Concern Period, referred to above, or otherwise; and (ii) the nature of the early stage clinical development and research and development activities that it is undertaking, where, by definition , there can be no assurance that it was be able to bring any of its proposed products to market. If the Company is unable to maintain adequate liquidity, future operations will need to be scaled back or discontinued. These conditions raise substantial doubt about the Company’s ability to continue as a going concern. The Company’s consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
| 91 |
Financial Operations Overview
Revenues
We do not have any approved products. Accordingly, we have not generated any revenue from the sale of products, and we do not expect to generate any such revenue unless and until we obtain regulatory approvals for, and commercialize any of, our product candidates. In the future, we will seek to generate revenue primarily from product sales and, potentially, regional or global collaborations with strategic partners, which may produce license fee income.
During the years ended December 31, 2019, 2020 and 2021, we had two collaboration agreements with global pharmaceutical companies. Revenue arose under these contracts as a result of (i) our recharging development costs incurred by us under those agreements to our partners and (ii) on upfront payments received under those collaboration agreements, which are taken to revenue on a straight-line basis over the estimated term over which the services promised will be provided. In addition, we are entitled to receive contractual payments, which would be recorded as revenue, when and if certain clinical trial performance milestones are met on partnered programs. Our collaborations are at a pre-clinical stage and there can be no assurance that we will receive any future milestone revenues.
Since inception through December 31, 2021, the Company has received £14.5 million ($19.6 million) in pre-clinical payments connected with CAR-T development deals with listed pharma companies (NIPRO, Japan: Bluebird Bio, US (now called 2seventy bio – NASDAQ (TSVT)).
Operating Expenses
We classify our operating expenses into two categories: research and development expenses and administrative expenses. Personnel costs, including salaries, benefits, bonuses and share-based payment expense, comprise a significant component of each of these expense categories. We allocate expenses associated with personnel costs based on the function performed by the respective employees.
Research and Development Expenses
The largest component of our total operating expenses since inception has been costs related to our research and development activities, including the preclinical and clinical development of our product candidates.
Research and development costs are expensed as incurred, with our development activities not yet at the point at which capitalization can occur under IFRS. Our research and development expense primarily consist of:
| ● | consumable costs related to research and development of pharmaceutical or biologic therapy products for preclinical studies and clinical trials; | |
| ● | costs related to manufacturing active pharmaceutical or biologic therapy products for preclinical studies and clinical trials; | |
| ● | salaries and personnel-related costs, including bonuses, benefits and any share-based payment expense, for our personnel performing research and development activities or managing those activities that have been out-sourced; | |
| ● | fees paid to consultants and other third parties who support our product candidate development; | |
| ● | third party costs incurred in connection with preclinical studies and clinical trials from investigative sites and contract research organizations, or CROs; | |
| ● | other costs incurred in seeking regulatory approval of our product candidates; |
| 92 |
| ● | costs of related office space allocated to our research and development function, materials and equipment; and | |
| ● | payments under our license agreements. |
The successful development of our product candidates is highly uncertain. Product candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical development, primarily due to the increased size and duration of later-stage clinical trials. In addition, the cost of development of our CAR-T range of products is likely to be substantially higher than costs incurred historically in the development of our unmodified products. Accordingly, we expect research and development costs to increase significantly for the foreseeable future as programs progress. However, we do not believe that it is possible at this time to accurately project total program-specific expenses through commercialization. We are also unable to predict when, if ever, material net cash inflows will commence from our product candidates to offset these expenses. Our expenditures on current and future preclinical and clinical development programs are subject to numerous uncertainties in timing and cost to completion.
The duration, costs and timing of clinical trials and development of our product candidates will depend on a variety of factors including:
| ● | the scope, rate of progress, results and expenses of our ongoing and future clinical trials, preclinical studies and research and development activities; | |
| ● | the potential need for additional clinical trials or preclinical studies requested by regulatory agencies; | |
| ● | potential uncertainties in clinical trial enrolment rates or drop-out or discontinuation rates of patients; | |
| ● | competition with other drug development companies in, and the related expense of, identifying and enrolling patients in our clinical trials and contracting with third-party manufacturers for the production of the drug product needed for our clinical trials; | |
| ● | the achievement of milestones requiring payments under in-licensing agreements; | |
| ● | any significant changes in government regulation; | |
| ● | the terms and timing of any regulatory approvals; | |
| ● | the expense of filing, prosecuting, defending and enforcing patent claims and other intellectual property rights; and | |
| ● | the ease, cost and ability to market, commercialize and achieve market acceptance for any of our product candidates, if approved. |
We track research and development expenses on a program-by-program basis for both clinical-stage and preclinical product candidates. Manufacturing, clinical trial and preclinical research and development expenses are assigned or allocated to individual product candidates. We do not allocate employee costs or facility expenses, including depreciation or other indirect costs, to specific programs because these costs are deployed across multiple programs and, as such, are not separately classified. We use internal resources primarily to oversee research and development as well as for managing our preclinical development, process development, manufacturing and clinical development activities.
Administrative Expenses
Administrative expenses consist of personnel costs, other administrative expenses and other expenses for outside professional services, including legal, audit and accounting services. Personnel costs consist of salaries, bonuses, benefits and share-based payment expense. Other administrative expenses include office space-related costs not otherwise allocated to research and development expense, professional fees and costs of our information systems. We anticipate that our administrative expenses will continue to increase in the future as we increase our headcount to support our continued research and development and potential commercialization of our product candidates. In the future, we expect to incur additional expenses as a public company, including expenses related to compliance with the rules and regulations of the SEC and Nasdaq, additional insurance expenses, and expenses related to investor relations activities and other administrative and professional services.
| 93 |
Change in fair value of convertible loan derivative
The gain/loss relates to the movement in the estimated fair value of the embedded derivative related to the issue of Notes from the point of recognition to the year end, calculated by using a Black Scholes option pricing model.
Finance Income
Finance income relates to interest earned on our cash and cash equivalents and short-term deposits.
Finance Costs
Finance costs include the effective interest charge accrued in relation to the Notes and interest expense representing the unwinding of discounted lease liabilities in respect of assets presented on our consolidated statement of financial position in accordance with IFRS 16 “Leases”.
Income Tax Credit
We are subject to corporate taxation in the United Kingdom. Due to the nature of our business, we have generated losses since inception. Our income tax credit recognized represents the sum of the research and development tax credits recoverable in the United Kingdom.
As a company that carries out extensive research and development activities, we benefit from the U.K. research and development tax credit regime and are able to surrender some of our losses for a cash rebate of up to 33.35% of expenditures related to eligible research and development projects. Qualifying expenditures largely comprise clinical trial and manufacturing costs, employment costs for relevant staff and consumables incurred as part of research and development projects. Certain subcontracted qualifying research and development expenditures are eligible for a cash rebate of up to 21.68%. A large portion of costs relating to our research and development, clinical trials and manufacturing activities are eligible for inclusion within these tax credit cash rebate claims.
We may not be able to continue to claim research and development tax credits in the future under the current research and development tax credit scheme because we may no longer qualify as a small or medium-sized company. However, we may be able to file under a large company scheme.
Tax losses that have not been utilized to offset taxable income or surrendered in connection with the aforementioned research and development tax credits are carried forward to be offset against future taxable profits.
In the event we generate revenues in the future, we may benefit from the UK government’s “patent box” initiative that allows profits attributable to revenues from patents registered in the United Kingdom or European Union or patented products to be taxed at a lower rate than other streams of revenue. The current rate of tax for relevant streams of revenue for companies receiving this relief is 10%.
Ukrainian Conflict
Currently the conflict between Ukraine and Russia does not have any direct effect on our operations, as they are generally conducted only in the United Kingdom. Currently, we believe the conflict will have only a general impact on our operations in the same manner as it is having a general impact on all businesses resulting from sanction and embargo regulations, possible shortages of goods that may be supplied from the Ukraine and Russia, and the inflationary results of the conflict.
| 94 |
Results of Operations
Comparison of the year ended December 31, 2021 and 2020
The following table summarizes the results of our operations for the twelve months ended December 31, 2021 and 2020:
| Year Ended December 31 | ||||||||||||
| 2021 | 2021 | 2020 | ||||||||||
| $’000 | £’000 | £’000 | ||||||||||
| Revenue | 2,672 | 1,979 | 1,979 | |||||||||
| Research and development expenses | (8,312 | ) | (6,157 | ) | (6,680 | ) | ||||||
| Administrative expenses | (2,778 | ) | (2,059 | ) | (2,207 | ) | ||||||
| Administrative expenses – costs related to preparing for a listing | (1,418 | ) | (1,050 | ) | - | |||||||
| Foreign exchange losses | (112 | ) | (83 | ) | - | |||||||
| Other income | 9 | 7 | 569 | |||||||||
| Change in fair value of convertible loan derivatives | (5,646 | ) | (4,182 | ) | - | |||||||
| Finance income | - | - | 1 | |||||||||
| Finance costs | (4,643 | ) | (3,439 | ) | (292 | ) | ||||||
| Loss before tax | (20,230 | ) | (14,984 | ) | (6,630 | ) | ||||||
| Income tax credit | 1,901 | 1,408 | 1,172 | |||||||||
| Net loss for the year and Total comprehensive loss | (18,329 | ) | (13,576 | ) | (5,458 | ) | ||||||
Revenue
Revenue was consistent at £2.0 million for both the year ended December 31, 2021 and December 31, 2020. The revenue in both periods is due to the satisfaction of performance obligations associated with upfront payments which are deemed to be satisfied over the estimated life of the services promised to be provided. There was no recharges of research and development spend to our collaboration partners, as those programs naturally progressed through phases of activity undertaken by partners rather than ourselves.
| 95 |
Research and development expenses
The table below summarizes our research and development expenses incurred by program:
| Year Ended December 31, | ||||||||||||
| 2021 | 2021 | 2020 | ||||||||||
| $’000 | £’000 | £’000 | ||||||||||
| Direct research and development expenses by program: | ||||||||||||
| Unmodified cell therapy programs | 1,530 | 1,133 | 606 | |||||||||
| Partner research and development programs | - | - | 71 | |||||||||
| Other research and development programs(2) | 124 | 92 | 223 | |||||||||
| Total direct research and development expense | 1,654 | 1,225 | 900 | |||||||||
| Research and development and unallocated costs: | ||||||||||||
| Personnel related (including share-based compensation) | 4,586 | 3,397 | 4,256 | |||||||||
| Indirect research and development expense (3) | 2,072 | 1,535 | 1,524 | |||||||||
| Total research and development expenses | 8,312 | 6,157 | 6,680 | |||||||||
| (1) | Unmodified cell therapy programs include OmnImmune® and ImmuniStim® | |
| (2) | Other research and development programs include expenditure on areas such as our CAR-T program, induced pluripotent stem cells (iPSCs) and the gammadelta1 (GD-T1) subtype. | |
| (3) | Indirect research and development expense includes property relates costs and depreciation and amortization. |
Research and development expenses decreased by 8% to £6.2 million for year ended December 31, 2021 from £6.7 million for the year ended December 31, 2020 reflecting the reduced level of staffing during the year offset by increased work on the ImmuniStim® program. Personnel costs reduced to £3.4 million for the year ended December 31, 2021 from £4.3 million for the year ended December 31, 2020 reflecting the reduced headcount from the second half of 2020 and in addition there were no share-based payment costs in the year ended December 31, 2021 as all options had fully vested by December 31, 2020. The share-based payment cost in the year ended D3ecmeber 31, 2020 was £0.6 million.
Administrative expenses
Administrative expenses decreased by 7% to £2.1 million for the year ended December 31, 2021 from £2.2 million for the year ended December 31, 2020. The decrease reflected lower levels of activity and no employee option share-based payment charges in the year ended December 31, 2021.
| 2021 | 2021 | 2020 | ||||||||||
| $’000 | £’000 | £’000 | ||||||||||
| Share based payment | - | - | 257 | |||||||||
| Employee related costs | 1,549 | 1,144 | 1,042 | |||||||||
| Legal & professional services | 942 | 697 | 646 | |||||||||
| Other expenses | 319 | 236 | 251 | |||||||||
| Foreign exchange movement | (24 | ) | (18 | ) | 11 | |||||||
| Total Administrative Expenses | 2,785 | 2,059 | 2,207 | |||||||||
Costs related to preparing for IPO of £1.1 million are also part of administrative expenses but are shown separately on the face of consolidated statements of comprehensive loss due to its material size.
| 96 |
Foreign exchange losses
These costs include unrealized and realized exchange differences in the year relate to retranslation of the US dollar denominated Convertible Loan Notes as at the year end totaling £0.1 million for the year ended December 31, 2021 (December 31, 2020: £Nil).
Other Income
Other income has decreased from £0.6 million in the year ended December 31, 2020 to £Nil for the year ended December 31, 2021. This is due to no receipts from employee furlough related government grants.
Change in fair value of convertible loan derivatives
The expense, totaling £4.2 million, for the year ended December 31, 2021 relates to the movement in the estimated fair value of the embedded derivatives related to the issue of Convertible Loan Notes from the point of recognition to the year end, calculated by using a Black Scholes option pricing model. There were no convertible loan notes in issue in 2020.
Finance Costs
Finance costs were £3.4 million for the year ended December 31, 2021 compared to £0.3 million for the year ended December 31, 2020. The increase reflected the effective interest rate calculated in respect of Convertible Loan Notes issued during the year ended December 31, 2021.
Income tax credit
The research and development tax credit of £1.4 million was 20% higher for the year ended December 31, 2021 compared to £1.2 million for the year ended December 31, 2020. This was due to higher levels of expenditure eligible for research and development tax credits.
After accounting for tax credits receivable, there were accumulated tax losses for carry forward in the United Kingdom of £7.5 million as of December 31, 2021 (December 31, 2020: £12.8 million). Unrecognized deferred tax assets totaling £3.3 million as of December 31, 2021 (December 31, 2020: £3.6 million) consist of temporary differences on tax losses and share-based compensation arrangements. No deferred tax asset is recognized in respect of accumulated tax losses or temporary differences on share-based compensation arrangements because future profits are not sufficiently certain.
Comparison of the years ended December 31, 2020 and 2019
The following table summarizes the results of our operations for the years ended December 31, 2020 and 2019:
| Year Ended December 31, | ||||||||||||
| 2020 | 2020 | 2019 | ||||||||||
| $ | £ | £ | ||||||||||
| Revenue | 2,672 | 1,979 | 3,427 | |||||||||
| Research and development expenses | (9,018 | ) | (6,680 | ) | (8,614 | ) | ||||||
| Administrative expenses | (2,979 | ) | (2,207 | ) | (3,015 | ) | ||||||
| Other income | 768 | 569 | 1,561 | |||||||||
| Finance income – interest | 1 | 1 | 22 | |||||||||
| Finance costs | (394 | ) | (292 | ) | (275 | ) | ||||||
| Loss before tax | (8,950 | ) | (6,630 | ) | (6,894 | ) | ||||||
| Income tax credit | 1,582 | 1,172 | 826 | |||||||||
| Net loss for the year | (7,368 | ) | (5,458 | ) | (6,068 | ) | ||||||
Revenue
Revenue decreased by 42% to £2.0 million for the year ended December 31, 2020 from £3.4 million for the year ended December 31, 2019. This reflected more research and development work being done in 2020 by our collaboration partners to progress programs, as those programs naturally progress through phases of activity to be undertaken by partners rather than ourselves, resulting in a corresponding reduction in incurred research and development spend which is recharged (as revenue to us) to our collaboration partners.
Research and development expenses
The table below summarizes our research and development expenses incurred by program:
| Year Ended December 31, | ||||||||||||
| 2020 | 2020 | 2019 | ||||||||||
| $ | £ | £ | ||||||||||
| Direct research and development expenses by program: | ||||||||||||
| OmnImmune® (TCB 008-001) | 382 | 283 | 977 | ) | ||||||||
| ImmuniStim® (TCB 008-002) | 436 | 323 | - | |||||||||
| Partner research and development programs | 96 | 71 | 945 | ) | ||||||||
| Other research and development programs (1) | 301 | 223 | 681 | ) | ||||||||
| Total direct research and development expense | 1,215 | 900 | 2,603 | ) | ||||||||
| Research and development and unallocated costs: | ||||||||||||
| Personnel related (including share-based compensation) | 5,773 | 4,276 | 4,594 | ) | ||||||||
| Indirect research and development expense(2) | 2,030 | 1,504 | 1,417 | |||||||||
| Total research and development expenses | 9,018 | 6,680 | 8,614 | ) | ||||||||
| (1) | Other research and development programs include expenditure on areas such as our CAR-T program, induced pluripotent stem cells (iPSCs) and the gammadelta1 (GD-T1) subtype. | |
| (2) | Indirect research and development expense includes property relates costs and depreciation and amortization. |
| 97 |
Research and development expenses decreased by 22% to £6.7 million for the year ended December 31, 2020 from £8.6 million for the year ended December 31, 2019. The reduction in direct research and development expenses of £1.7 million in 2020 reflected the impact of a reduced level of clinical activity due to the impact of the coronavirus pandemic of £2.0 million offset by increased expense related to the new clinical program in response to the pandemic of £0.3 million. Personnel costs reduced to £4.3 million for the year ended December 31, 2020 from £4.6 million for the year ended December 31, 2019 reflecting the reduced headcount during 2020. Indirect research and development expense, which contains a number of fixed costs such as facility and property expenditure increased to £1.5 million for the year ended December 31, 2020 from £1.4 million for the year ended December 31, 2019. Our research and development expenses are highly dependent on the phases of our research projects and therefore fluctuate from year to year.
Administrative expenses
Administrative expenses decreased by 27% to £2.2 million for the year ended December 31, 2020 from £3.0 million for the year ended December 31, 2019. Similarly, to research and development expenses, the reduction reflected a reduced level of activity to the impact of the pandemic and we expect these costs to increase in 2021.
Other Income
Other income has decreased from £1.6 million in the year ended December 31, 2019 to £0.6 million for the year ended December 31, 2020. This is due to a reduced amount of program related grant claims being awarded and recognized during 2020. During the year ended December 31, 2020 the Company recognized employee furlough related government grants totaling £0.5 million.
Finance Income – Interest
Finance income – interest consisted of bank interest earned on cash balances and short-term deposits. Finance income – interest was less than £0.1 million for the year ended December 31, 2020 and the year ended December 31, 2019. Interest income reduced during 2020 due to lower levels of short-term deposits and cash at bank. Interest income consisted of bank interest earned on cash balances and short-term deposits.
Finance Costs
Finance costs related to sale and leaseback finance costs and interest computed on the liabilities associated with right of use assets. Finance costs were less than £0.3 million for the year ended December 31, 2020 and the year ended December 31, 2019. Interest expenses increased by 6% in 2020 reflecting a full year of lease costs from additional property leases established during the prior year.
Income tax credit
The research and development tax credit increased by 42% to £1.2 million for the year ended December 31, 2020 from £0.8 million in the same period in 2019. The increase was driven by the increase in the proportion of those expenditures that are eligible for research and development tax credits.
Critical Judgments in Applying Our Accounting Policies
In the application of our accounting policies, we are required to make judgments, estimates, and assumptions about the value of assets and liabilities for which there is no definitive third-party reference. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from these estimates.
Our estimates and assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimate is revised if the revision affects only that period, or in the period of the revisions and future periods if the revision affects both current and future periods.
The following are our critical judgments, except those involving estimation uncertainty, that we have made in the process of applying our accounting policies and that have the most significant effect on the amounts recognized in our consolidated financial statements included elsewhere in this Annual Report.
Going Concern
Our evaluation of our ability to continue as a going concern requires us to evaluate our future sources and uses of cash sufficient to fund our currently expected operations in conducting research and development activities one year from the date our consolidated financial statements are issued. We evaluate the probability associated with each source and use of cash resources in making our going concern determination. The research and development of cell therapies is inherently subject to uncertainty.
Management believes that its existing cash balances coupled with planned further financings during 2022 will be sufficient to fund the current operating plans for at least the twelve month period following the filing date of this Annual Report. Should the additional planned financings not occur as expected, management will implement alternative arrangements and such arrangements could have a potentially significant negative impact on the current net asset value of the Group. These alternatives include: (1) raising additional capital my means other than those planned through equity and/or debt financings; (2) entering into new commercial relationships to help fund future clinical trial costs (i.e. licensing and partnerships); (3) reducing and/or deferring discretionary spending on general corporate overheads and one or more of our research and development and / or clinical programs; and/or (4) restructuring operations to change our overhead structure and make use of our manufacturing facilities to generate revenues from through third party manufacturing contracts. In the medium term the Company’s future liquidity needs, and ability to address those needs, will largely be determined by the success of its product candidates and key development and regulatory events and its decisions in the future.
Further detail about the Company’s ability to continue as a going concern are described in Note 1 to the consolidated financial statements.
| 98 |
Revenue from contracts with customers
Identification of contracts with pharma partners
The Company has entered into collaboration agreements with a number of parties. Application of IFRS 15 “Revenue from contracts and customers” on collaboration agreements requires judgement around whether these contracts were within the scope of IFRS 15.
The Company’s core business is around researching and developing immunotherapies and the contracts entered into with pharma partners are consistent with those objectives and the outputs are in line with the Company’s ordinary activities.
The contracts with pharma partners do not involve sharing the risks and benefits of a joint arrangement in the sense of IFRS 11 “Joint arrangements”.
In light of work being undertaken with pharma partners, and the fact that these agreements have commercial substance with clearly defined milestones and rights and obligations for each party, management concluded that these collaboration agreements meet the definition of a contract with a customer and fall within the scope of IFRS 15.
Identification of performance obligations in contracts
The collaboration agreements entered into by the Company include obligations to fulfil the research and development programs. The Company identified, from reviews of the relevant agreements, that there are no specific obligations but an implied performance obligation to deliver each overall contracted research and development program. Reflecting the broad nature of these obligations, spanning the full duration of the contract, the obligations are satisfied over the expected duration of the relevant contract.
Determination and allocation of the transaction price
The collaboration agreements include a number of elements of consideration and are allocated to the satisfaction of the relevant obligation.
The Company can receive upfront payments as part of the consideration. The Company has determined that upfront payments are in connection with the performance of the research and development program and are satisfied during the duration of the contract.
The business is entitled to receive contractual milestone payments on achievement of certain performance obligations, with revenue being recognized in the same way. The relevant transaction price is allocated to the related milestone.
Convertible loan redemption date
The Group calculates the effective interest rate (“EIR”) to consider the potential repayment at redemption date by reference to the face value amount and including the 5% of interest rate in each relevant cash outflow period. At the time of a listing, 50% of the face value of loan notes in issue at the time (including interest accrued to date) convert to equity in the listed entity with the remaining loan notes are repayable or convertible at the loan note holders’ option in two equal tranches at 90 days and 180 days after the listing date. For the purpose of calculating the EIR, management estimated as at December 31, 2021, the listing date to be on or around January 18, 2022.
Embedded derivative assumptions
The estimated fair value of the embedded derivatives related to the issue of convertible loan notes at the point of recognition and at the period end was calculated by using a Black Scholes option pricing model.
Management determined the share price used in the fair value calculation in line with the methods discussed in Note 2 in connection with the ‘Valuation of ordinary shares’, in particular noting the recent valuation obtained from advisers in connection with the planned IPO. As a privately held company, the Group’s share price does not have sufficient historical volatility to adequately assess the fair value of the embedded derivative. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that a volatility of 80% was appropriate for the valuation of embedded derivatives in in existence as at December 31, 2021.
The expected life of the embedded derivative was directly linked to expected redemption dates of the convertible loan note, as noted above.
The Black-Scholes option pricing model requires the use of the risk-free rate of the currency in which the convertible loan note is denominated (US dollars). The Group has applied the appropriate risk-free rate, US treasury bond yields as at the respective redemption dates.
Key Sources of Estimation Uncertainty
The key assumptions concerning the future, and other key sources of estimation uncertainty at the balance sheet date, that have a significant risk of causing a material adjustment to the carrying amounts of assets and liabilities within the next year are discussed below.
Revenue from contracts with customers
Timing of revenue recognition
Revenue from upfront payments in connection with collaboration agreements is recognized over the estimated term over which the services promised will be provided. This term was estimated by management at the inception of each contract and evaluated at the year end. The estimated time to complete as at the December 31, 2021 is 23 months.
| 99 |
The resulting deferred income liabilities are disclosed in the consolidated financial statements attached to this Annual Report. Due to the uncertainty around the time to complete multi-year collaboration programs it is possible that the estimated terms may be extended. If the estimated term of the current contracts had been adjusted by one year, then it would be expected that the corresponding revenue for the year ended December 31, 2021 would have decreased by £0.5 million and deferred income liabilities would have increased by £0.5 million as at December 31, 2021. The business is entitled to receive contractual milestone payments on achievement of certain performance obligations. Due to significant uncertainties associated with the achievement of contractual milestones, no revenue has been recognized to date from milestone payments and these will be recognized when the milestones are certain to occur.
Valuation of ordinary shares
As there has been no public market for the Group’s ordinary shares until February 10, 2022, the date of our initial public offering, the estimated fair value of the ordinary shares has been determined by management, considering the most recently available third-party valuations of the Group’s ordinary shares, and the assessment of additional objective and subjective factors that it believed were relevant and which may have changed from the date of the most recent valuation through the date of the grant.
After considering the Market Approach, the Income Approach and the Asset-based Approach, we utilized the Market Approach to determine the estimated fair value of our ordinary shares based on management’s determination that this approach was most appropriate for a clinical-stage biopharmaceutical company at this point in its development, using the option-pricing method (“OPM”). Consideration was given to the American Institute of Certified Public Accountants’ Practice Aid: “Valuation of Privately-Held Company Equity Securities Issued as Compensation,” or the Practice Aid, in addition to input from management, the likelihood of completing an IPO and recent transactions with investors.
Once a public trading market for the ADSs, which represent our ordinary shares, has been established in connection, it will no longer be necessary to estimate the fair value of our ordinary shares in connection with our accounting for share-based payment expenses, as the fair value of our ordinary shares will be determinable by reference to the trading price of the ADSs on Nasdaq.
Share option and other share-based payment assumptions
The determination of the value of share-based payments requires management to use professional expertise to arrive at assumptions to be used to calculate the value of the share-based payment. The estimated fair value of the options outstanding in the period was calculated by applying a Monte Carlo simulation for those options issued in 2020 and a Black Scholes Model for those options issued in prior periods. The most appropriate approach is selected with reference to the share capital structure at the time of grant and the directors need to use judgement in setting the key assumptions. Further details are included in the consolidated financial statements attached to this Annual Report.
The Company determines the share price used in the fair value calculation in line with the methods discussed in above in connection with the “Valuation of ordinary shares”. As a privately held company, the Company’s share price does not have sufficient historical volatility to adequately assess the fair value of the share option grants. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that volatility of 70% was appropriate for the valuation of our share options.
The expected life of the option, beginning with the option grant date, was used in valuing our share options. The expected life used in the calculation of share-based payment expense is the time from the grant date to the expected exercise date. The life of the options, which is a subjective estimate that can materially alter the valuation, depends on the option expiration date, volatility of the underlying shares and vesting features.
IFRS 2 “Share-based Payment” requires the use of the risk-free rate of the country in which the entity’s shares are principally held with a remaining term equal to the expected life of the option. This should also be the risk-free interest rate of the country in whose currency the exercise price is expressed. The Company has applied the appropriate risk-free rate, based on 4-year, 3-year and 2-year UK government bond yields as at the respective grant dates.
| 100 |
Convertible loan redemption date
The Company calculates the effective interest rate (“EIR”) to consider the potential repayment at redemption date by reference to the face value amount and including the 5% of interest rate in each relevant cash outflow period For the purpose of calculating the EIR, management estimates the listing date to be on or around January 18, 2022.
Embedded derivative assumptions
The estimated fair value of the embedded derivatives related to the issue of convertible loan notes at the point of recognition and at the year end was calculated by using a Black Scholes option pricing model.
The Group determined the share price used in the fair value calculation in line with the methods discussed in Note 2 in connection with the ‘Valuation of ordinary shares’, in particular noting the recent valuation obtained from advisers in connection with the planned IPO. As a privately held company, the Group’s share price does not have sufficient historical volatility to adequately assess the fair value of the embedded derivative. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that a volatility of 80% was appropriate for the valuation of embedded derivatives in in existence as at December 31, 2021.
The expected life of the embedded derivative was directly linked to expected redemption dates of the convertible loan note, as noted above.
The Black-Scholes option pricing model requires the use of the risk-free rate of the currency in which the convertible loan note is denominated (US dollars). The Group has applied the appropriate risk-free rate, US treasury bond yields as at the respective redemption dates.
Convertible loan
During 2021, the Group issued convertible loan notes with a face value of $17,657,808 (£13,051,821 based on the exchange rate as at December 31, 2021) in exchange for $8,768,904 (£6,481,561) in cash. These notes require the payment of mandatory annual interest coupons of 5% p.a. and mature, unless previously repaid or converted in shares on February 15, 2022.
In the event of and at the time of an IPO, 50% of the face value of the outstanding Convertible Loan Notes (including interest accrued to date), and any further balance as elected by the noteholders, will convert into shares at a conversion price, which is the lower of (a) the price per share calculated on a fully diluted basis (based on the number of shares in issue and vested share options immediately prior to the IPO being approved by the shareholders) on an assumed entity valuation of $120,000,000 and (b) the listing price. The remaining amount due under the loan notes are repayable at par or convertible (on the same value) into shares in the listed entity at the loan note holders’ option in two equal tranches at 90 days and 180 days after the listing date.
At the time of our initial public offering on February 10, 2022, loan notes totaling $13,447,012 converted into 3,164,015 ADSs and 6,328,030 Warrants at a combined issue price of $4.25.
In the event of an act of default (including if the Group does not list despite its and its bankers’ efforts before February 15, 2022) the outstanding notes become immediately repayable at their face value.
The convertible loan has been recognized as a debt instrument with a contingently conversion option separately accounted for as an embedded conversion option derivative.
| (i) | The convertible loan debt host instrument’s initial fair value is the residual amount of the consideration received, net of attributable costs of £100,000, after separating out the fair value of the embedded conversion option derivative. The loan is subsequently measured at its amortized cost in accordance with IFRS 9 – Financial Instruments. It is presented as a financial liability in the consolidated statement of financial position. Management calculates the effective interest rate (“EIR”) to consider the potential repayment at redemption date by reference to the face value amount after taking into account the 5% interest rate. The calculated effective daily interest rate is up to 28% given the significant value of the embedded conversion option on issuance of the instrument. | |
| (ii) | The embedded conversion option derivative was initially measured at fair value and is subsequently remeasured to fair value at each reporting date. Under IAS 32 Financial Instruments: Presentation, this derivative could have been classified as a component of equity only if in all cases the contract would be settled by the Group delivering a fixed number of its own equity instruments in exchange for a fixed amount of cash or debt redemption. However, the convertible instrument included a conversion feature resulting in settlement in a variable number of shares and consequently, none of the instrument comprises an equity component. As a result, the derivative is presented in the statement of financial position as a liability in accordance with IFRS 9 and IAS 32. Changes in the fair value (gains or losses) of the derivative at the end of each period are recorded in the consolidated statements of comprehensive loss. |
| 101 |
The value of the embedded derivative is remeasured at fair value at each reporting date (based on a Black-Scholes valuation model) with recognition of the changes in fair value in the consolidated statements of comprehensive loss in accordance with IFRS 9. The inputs associated with calculating the fair value of the embedded derivative are considered to be Level 3 (inputs not based on observable market data) as defined by IFRS 7 – Financial instruments: Disclosures and therefore the valuation of the conversion option is a level 3 valuation. The significant inputs used in the valuation are:
| The model inputs were as follows: | ||||
| 2021 | ||||
| Exercise price in USD | $ | 4.82 | ||
| Share price in USD | 8.00 | |||
| Time to maturity | 1 to 7 months | |||
| Expected volatility | 71% - 80 % | |||
| Risk free interest rate (US treasury bond) | 0.08 | % | ||
| Dividend yield | - | |||
| Probability, as at the reporting date, of IPO completion | 75 | % | ||
Emerging Growth Company
The federal securities laws provide that an emerging growth company may take advantage of an extended transition period for complying with new or revised accounting standards. As an emerging growth company, we have irrevocably elected not to take advantage of the extended transition period for implementation of new or revised accounting standards and, as a result, we will comply with new or revised accounting standards on the relevant dates on which adoption of such standards is required for non-emerging growth public companies.
In addition, we intend to rely on the other exemptions and reduced reporting requirements for emerging growth companies. Subject to certain conditions, we are entitled to rely on certain exemptions as an “emerging growth company,” we are not required to, among other things, (i) provide an auditor’s attestation report on our system of internal controls over financial reporting pursuant to Section 404(b), (ii) provide all of the compensation disclosure that may be required of non-emerging growth public companies under the Dodd-Frank Wall Street Reform and Consumer Protection Act, (iii) comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements (auditor discussion and analysis), and (iv) disclose certain executive compensation-related items such as the correlation between executive compensation and performance and comparisons of the chief executive officer’s compensation to median employee compensation. These exemptions will apply for a period of five years following the completion of our initial public offering, or December 2026, or until we no longer meet the requirements of being an emerging growth company, whichever is earlier.
Recently Issued and Adopted Accounting Pronouncements
For information on the standards applied for the first time as of January 1, 2020 and 2021, please refer to our consolidated financial statements as of December 31, 2020 elsewhere in this Annual Report.
| 102 |
| B. | Liquidity and Capital Resources |
Overview
For the years ended December 31, 2021 and December 31, 2020, we incurred net losses of £13.6 million and £5.5 million, respectively. We used £5.3 million of cash in operating activities in the year ended December 31, 2021 and used £3.4 million of cash in operating activities for the year ended December 31, 2020.
As of December 31, 2021, and December 31, 2020, we had cash and cash equivalents of £1.6 million and £0.7 million, respectively. From incorporation through to December 31, 2021, we have financed our operations primarily through private placements of equity securities, convertible loans, government grants, research and development tax credits, and receipts from partner for collaborative research and development services totaling £47.7 million. On February 15, 2022, the Company completed its IPO on Nasdaq, raising net proceeds of $14.5 million. Management believes that the net proceeds from this offering and the existing cash and cash equivalents together with future planned fundraisings during 2022 will be sufficient to fund our operating plans for at least rwelve months adter the filing dte of this Annual Filing.
If we obtain regulatory approval to advance any of our GD-T cell therapeutic candidates into pivotal clinical trials or to commercialization, we will incur significant research and development expenses, and also commercialization expenses related to product sales, marketing, manufacturing and distribution and additional funding would be required. Where appropriate, we will seek to fund our operations through milestone payments under our agreements with collaboration partners and additional equity financings.
Cash Flows
The following tables summarize the results of our cash flows for the below respective periods:
| Year Ended December 31, | ||||||||||||
| 2021 | 2021 | 2020 | ||||||||||
| $’000 | £’000 | £’000 | ||||||||||
| Consolidated Cash Flow Statement: | ||||||||||||
| Net cash flows used in operating activities | (7,534 | ) | (5,581 | ) | (3,432 | ) | ||||||
| Net cash flows used in investing activities | (193 | ) | (143 | ) | (205 | ) | ||||||
| Net cash flows from financing activities | 8,807 | 6,525 | 3,430 | |||||||||
| Net increase in cash and cash equivalents | 1,080 | 801 | (207 | ) | ||||||||
Operating Activities
Net cash used in operating activities was £5.6 million for the year ended December 31, 2021. The loss before taxation for the year ended December 31, 2021 was £14.9 million, which is offset by noncash items of £1.0 million, research and development tax credit receipts of £1.2 million, £7.2 million of costs related to the interest charge on the convertible loan note and movement in the embedded derivative in the income statement and changes in working capital of £0.1 million. The noncash items consisted primarily of finance costs, changes in fair value of a derivative liability, depreciation and amortization. The changes in working capital in the year reflected an increase in trade and other receivables, a decrease in deferred income offset by an increase in trade and other payables.
Net cash used in operating activities was £3.4 million for the year ended December 31, 2020. The loss before taxation for the year ended December 31, 2020 was £6.6 million, which is offset by noncash items of £1.8 million, £1.2 million for tax credit receipts and changes in working capital of £0.1 million. The noncash items consisted primarily of finance costs, depreciation, amortization and share based payments. The changes in working capital in the year reflected a decrease in trade and other receivables and an increase in trade and other payables offset by a decrease in deferred income.
Investing Activities
Net cash used in investing activities was £0.1 million and £0.2 million for the year ended December 31, 2021 and year ended December 31, 2020, respectively. These amounts relate primarily to purchases of property, plant and equipment related to our facility and patent filing costs.
| 103 |
Financing Activities
Net cash from financing activities was £6.5 million and £3.4 million for the year ended December 31, 2021 and year ended December 31, 2020, respectively.
For the year ended December 31, 2021, these amounts consisted of net proceeds from the issue of Convertible Loan Notes (£6.0 million), together with proceeds from sale of own shares (£0.3 million) offset by the repayment of lease liabilities (£0.1 million). For the year ended December 31, 2020, these amounts consisted of proceeds from the issue of ordinary share capital (£3.9 million) offset by the repayment of lease liabilities (£0.4 million)
Funding Requirements
We expect our expenses to increase substantially in connection with our ongoing activities, particularly as we advance the preclinical activities and clinical trials of our product candidates. Our expenses will increase as we (i) advance our product candidates through phases of clinical development and, potentially, registration, (ii) fund our research and development activities to further expand our GD-T cell technologies and develop future product candidates and follow-on versions of our more advanced product candidates, (iii) fund our manufacturing activities and the expansion of our plant to support our ongoing and future clinical trials and potential commercial launch; and (iv) fund our general operations.
Since February 10, 2022, we have been a publicly traded company and will incur significant legal, accounting and other expenses that we were not required to incur as a private company. In addition, the Sarbanes-Oxley Act of 2002, as well as rules adopted by the SEC and The Nasdaq Stock Market, requires public companies to implement specified corporate governance practices that are currently inapplicable to us as a private company. We expect these rules and regulations will increase our legal and financial compliance costs and will make some activities more time-consuming and costly.
We expect that our cash resources received from the IPO together with future planned fundraisings in 2022 will enable us to fund our planned operating expenses and capital expenditure requirements for at least twelve months after the filing of this Annual Report. We have based these estimates on assumptions that may prove to be wrong, and we could utilize our available capital resources sooner than we expect. We will require additional capital to continue to conduct our business and implement our business plans.
Because of the numerous risks and uncertainties associated with research, development and commercialization of pharmaceutical product candidates, we are unable to estimate the amount of our future working capital requirements, which will depend on and are likely to increase significantly as a result of many uncertain factors, including:
| ● | the scope, progress, outcome and costs of our clinical trials and other research and development activities; | |
| ● | the costs, timing, receipt and terms of any marketing approvals from applicable regulatory authorities; | |
| ● | the costs of future sales and marketing activities, including cost of product sales, medical regulatory affairs, marketing, manufacturing and distribution, for any of our product candidates for which we receive marketing approval; | |
| ● | the amount and timing of the receipt of any future revenue from commercial sale of our products, should any of our product candidates receive marketing approval and become successful in the market; | |
| ● | the impact of the COVID-19 pandemic on our ability to progress research and development and clinical trials; | |
| ● | the costs and timing of hiring new employees to support our future growth; | |
| ● | the costs of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending intellectual property-related claims; and |
| 104 |
| ● | the cost of and extent to which we in-license or acquire additional product candidates or technologies. |
Until such time, if ever, that we can generate product revenue sufficient to achieve profitability, we expect to finance our future cash needs through equity offerings and debt and a combination thereof, including securities convertible into ordinary shares and through development collaborations with partners.
To the extent that we raise additional capital through the sale of equity, our shareholders’ ownership interest will be diluted.
If we raise additional funds through other third-party funding, collaborations agreements, strategic alliances, licensing arrangements or marketing and distribution arrangements, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or grant licenses on terms that may not be favorable to us.
If we are unable to raise additional funds when needed, we may be required to delay, limit, reduce or terminate our product development or future commercialization efforts or grant rights to develop and market products or product candidates that we would otherwise prefer to develop and market ourselves. If we raise funding through borrowings, we may have to enter into onerous covenants which may adversely impact our operations and our ability to obtain further funding.
There is no assurance that we will be able to raise any further funding, or if further funding is offered, it will be on terms that are acceptable to us and may bring dilution which is unacceptable to our shareholders.
| C. | Research and Development, Patents and Licenses, etc. |
Full details of our research and development activities and expenditures are given in “Item 4. Information on the Company–B. Business” and “Item 5A. Operating Results” within this Annual Report.
| D. | Trend Information |
See “Item 5A. Operating Results” within this Annual Report.
| E. | Off-Balance Sheet Arrangements |
Not applicable.
| F. | Tabular Disclosure of Contractual Obligations |
The following table summarizes our contractual obligations as of December 31, 2021 and the effects that such obligations are expected to have on our liquidity and cash flows in future periods:
| December 31, 2021 | Carrying amounts | Total | 2 months or less | 2-12 months | 12-24 months | More than 2 years | ||||||||||||||||||
| Financial liabilities | £ | £ | £ | £ | £ | £ | ||||||||||||||||||
| Trade payables | 1,422,393 | 1,422,393 | 1,422,393 | - | - | - | ||||||||||||||||||
| Convertible loan | 13,731,864 | 20,359,893 | 10,088,496 | 10,271,397 | ||||||||||||||||||||
| Other payables | 2,681,223 | 2,681,223 | 831,029 | 1,850,194 | - | - | ||||||||||||||||||
| 17,835,480 | 24,463,509 | 12,341,918 | 12,121,591 | - | - | |||||||||||||||||||
| 105 |
Lease liabilities and similar
Amounts shown as lease liabilities and similar reflect minimum payments due for our leases of office, laboratory and manufacturing space and finance leases in respect of certain plant and equipment. We entered into a lease for our corporate headquarters in April 2014 and, as part of this agreement, exercised an option to lease additional space in January 2017 and March 2019. The overall lease expires in February 2029.
Convertible Loan Notes
In respect of the Convertible Loan Notes recognised as a financial liability as at December 31, 2021, a proportion of the Loan under the loan agreement is expected to convert to equity and will not result in a cash outflow.
Other commitments
We enter into contracts in the normal course of business with third parties who support us in the conduct of certain specialist aspects of clinical trials and preclinical research studies and testing. These contracts are generally cancellable by us upon prior notice. Payments due upon cancellation consist only of payments for services provided or expenses incurred, including noncancelable obligations of our service providers, up to the date of cancellation. These payments are not included in the preceding table, as the amount and timing of such payments are not known.
We have not included any contingent payment obligations that we may incur upon achievement of clinical, regulatory and commercial milestones, as applicable, or royalty payments that we may be required to make under in-licensing agreements which we have or may enter into which could be payable if any of our products generate future sales or license revenue as the amount, timing and likelihood of such payments are not known and are not anticipated in the near term or before we generate significant revenues.
| G. | Safe Harbor |
See the section titled “Information Regarding Forward-Looking Statements” at the beginning of this Annual Report.
| Item 6. | Directors, Senior Management and Employees |
| A. | Directors and Senior Management |
The following table sets forth the names, ages and positions of our executive officers and directors:
| Name | Age | Position | ||
| Dr Michael Leek | 62 | Executive Chairman of the Board (Founder) and Director | ||
| Bryan Kobel | 42 | Chief Executive Officer and Director | ||
| Martin Thorp | 70 | Chief Financial Officer and Director | ||
| Angela Scott | 58 | Chief Operating Officer (Founder) | ||
| Dr Mark Bonyhadi | 68 | Director (Non-executive) | ||
| James Culverwell | 65 | Director (Non-executive) | ||
| Arlene Morris | 70 | Director (Non-executive) | ||
| Edward Niemczyk | 41 | Director (Non-executive) |
| 106 |
Senior Management
Dr Michael Leek (Executive Chairman and Director)
Michael Leek, Ph.D., MBA has served as our Chief Executive, co-founder and executive board member since July 2013. Prior to this, Dr. Leek served in senior management and board roles with, Intercytex plc, a cell therapy company he co-founded. While at Intercytex, Dr. Leek was involved in clinical development of cell therapies to treat chromic dermal wounds. Early in his career, he held roles of increasing responsibility at Smith and Nephew from 1989 to 1999 as leader of the Tissue Repair Enabling Technology team. Dr. Leek holds a Ph.D. (Forensic Medicine) from the University of Leeds. He has acted as an honorary lecturer at the School of Medical Sciences, University of Aberdeen since January 2014.
Bryan Kobel (Chief Executive Officer and Director)
Bryan Kobel has served as our Chief Executive Officer since June 2021. Prior to joining TC BioPharm he served as Managing Director at EF Hutton from October 2020 as the head of healthcare investment banking. From June 2018 to October 2020, Mr. Kobel was Managing Director and head of healthcare/capital markets at the Alberleen Group where he led deal origination and structuring, as well as leading the sales efforts for transactions across the Healthcare and Technology sectors. From April 2017 to June 2018, he was Head of Capital Markets at R.F. Lafferty & Co. From March 2012 to April 2017, Mr. Kobel was Managing Director, Capital Markets at Laidlaw & Company. Mr. Kobel holds a BA degree from Franklin & Marshall College and held the FINRA licenses Series 7, 63, 82, 79 and 24.
Martin Thorp (Chief Financial Officer and Director)
Martin Thorp has been a member of the Board of directors since March 2016 and has served, in an executive capacity, as the Chief Financial Officer since March 2019. From December 2014, Martin was founder (and from 2018 chairman) of a life science financial advisory firm, Copernican Capital Partners Limited (formally NCL Corporate Finance Limited), where he acted as corporate finance adviser to and investor in, several disruptive life science companies. Martin was also a co-founding director of a life science advisory and investment firm NCL Technology Ventures from 2014 to 2018. He was a director of Discovery Park Technology Investments (GP) Limited (and associated investment companies) from September 2016 until July 2018. Martin holds a B.A. in business finance from the University of Kent and qualified as a Chartered Accountant with Arthur Andersen & Co in London in 1977 and became a Fellow of the Institute of Chartered Accountants in England and Wales (ICAEW) in 1986. He was a partner in Arthur Andersen & Co from August 1985, and served in several roles including founder and global managing partner of Arthur Andersen’s international corporate finance business, based latterly in New York. He retired from professional practice in 2002 and consequently ceased to be a member of ICAEW in 2004.
Angela Scott (Chief Operating Officer)
Angela Scott is a co-founder of the Company and served as an executive director of the Company from December 2018 until her resignation from the Board on October 22, 2021. She has served as our Chief Operating Officer since January 2014. Prior to this Ms. Scott was Director of Operations at Angel Biotechnology plc from 2005 to 2012 where she transitioned several cell therapies into clinical trials which included first in man stem cell product for the treatment of stroke. From 2003 to 2004, she served as Development Manager for Cell Culture and Diagnostics at Excell Biotechnology. Prior to this, she served as Senior Research Associate, from 1992 to 2003, at PPL Therapeutics, where she was part of the team that cloned ‘Dolly the sheep’. Ms Scott held roles with increasing responsibility with Imperial Cancer Research Fund from 1981 to 1992. She has acted as an advisory board member of both the ATMP Manufacturing Community and Scottish Stemcell Network. Ms. Scott has a BSc in Biological Sciences from Napier University, Edinburgh.
| 107 |
Non-Executive Directors
Dr Mark Bonyhadi (Director)
Mark Bonyhadi, PhD has served as a director since February 2022. He is a Senior Advisor at Qiming Venture Partners USA. Prior to joining Qiming in December 2018, Mark held positions of Vice President of Research, Head of Academic Affairs, and Vice President of Process Research Sciences from 2013-2018 at Juno Therapeutics. From 2006-2013, Mark was Director of Global Business Development for Cell Therapy at Invitrogen, which was merged with Applied BioSystems, to create Life Technologies, which subsequently was acquired by Thermo-Fisher. Mark was responsible for identifying and implementing business opportunities aligned with the Lifetech/Invitrogen/Thermo cellular medicine portfolio, participating, and leading in the launch of the Cell Therapy Systems (CTS™) product line optimized for cell therapy applications, as well as working with academia and industry to accelerate the development of novel cell and/or gene-based therapies. From 1997-2005, Mark served as Director and later Vice President of Research at Xycte Therapies, a T cell therapy company treating cancer, infectious disease, and autoimmunity. Prior to that, Mark was a senior scientist at SyStemix, a biotech company developing hematopoietic stem cell-based therapies for treating cancer, where he did his postdoctoral training. Mark is a former Chair and current member of the Industry Liaison Committee for the American Society for Gene and Cell Therapy (ASGCT). Mark received a B.A. from Reed College, Portland, OR (1982) and a PhD from University of California at Berkeley (1990), where he studied T cell immunology, and identified the first delta chain protein product of the recently discovered gamma/delta T cell. Since graduating from UC Berkeley, Mark has been focused on the development of commercially viable approaches and business strategies for bringing cell therapies, gene-modified cell therapies, and regenerative medicine from the bench to the clinic, and into commercial use over the past three decades.
James Culverwell (Director)
James Culverwell has served as a director since February 2022. He currently is also a non-executive director and chairman of the audit committee of Innocoll Holdings plc (a collagen-based drug delivery company) from 2013 until 2017 during which period it relocated from Dublin to Germany and ultimately listed on Nasdaq (INNL). Between 2016 and 2019 he was a non-executive director and chairman of the audit committee of Amryt Pharmaceuticals plc, a commercial and research-based company specializing in rare diseases, which during his tenure listed on the Dublin STX and the London AIM markets and acquired Aegerion, a Nasdaq listed company. Since its foundation in 2006, Mr Culverwell has been a non-executive director and chairman of the audit committee of Safeguard Biosystems, a private company providing high throughput, multiplexed, molecular diagnostic tests and now generating commercial revenues. Since 2013 Mr Culverwell has been Chief Executive and is currently Chairman of HOX Therapeutics, a UK based private company researching early-stage treatments for prostate cancer. Since 2021 he has been a director and the chairman of the audit committee of Quoin Pharmaceuticals Inc., which is initiating clinical trials in a treatment for rare skin diseases. Since 2010 he has served as a healthcare investment consultant to a large secondary fund, where he performs due diligence on life science investment candidates. In 2005 Mr Culverwell established a corporate advisory firm, advising small life science companies on fund raising and larger companies on strategy and investor relations. From 1994-2004 Mr Culverwell was VP and Global Administrator Healthcare Equity Research Merrill Lynch/Bank of America and from 1982-94 he was Director and Head of European Healthcare and Pharmaceutical Equity Research at Hoare Govett/ABN Amro. He holds an MSc (Hons) in biology from the University of Aberdeen.
Arlene Morris (Director)
Arlene Morris has served as a director since February 2022. She currently serves (since July 2019) as a non-executive director of the following companies: Cogent Biosciences, Inc. (NASDAQ: COGT) (since July 2019), where she is the chair the compensation committee and is a member of the audit committee and the nominating and corporate governance (‘N&G’) committee; Viridian Therapeutics, Inc. (NASDAQ: VRDN) (since January 2018), where she is a member of the audit, pricing and N&G Committees; and Palatin Technologies, Inc. (NYSE: PTN) (since 2015), where she is a member of the compensation and N&G committees. Ms Morris has also served as a non-executive director at the following companies: Neovacs SA (2011 to 2021), Dimension Therapeutics, Inc. (2015-018), Biodel, Inc. (2012-2015), MediciNova, Inc. (2006-2013). Ms Morris is an emeritus member of the board of directors at the Medical University of South Carolina (‘MUSC’) (since 2012) and is also (since 2016) a member of the board of trustees of Carlow University (PA). She has also served as a member (including of the executive committee) of the Biotechnology Innovation Origanisation (‘BIO’), which is a biotechnology industry advocacy organization; and of the charitable organization, the Humane Society of Silicon Valley (including chair of the audit committee). She has held senior executive management roles in the pharmaceutical group Johnson & Johnson including business development, product development, strategic marketing, product management and sales management.
| 108 |
Edward Niemczyk (Director)
Edward Niemczyk has served as a director since February 2022. He is a Partner at Bridges Fund Management, Ltd (‘Bridges’), a private equity firm focused on sustainable and impact investing. He has been with Bridges’ U.S. Sustainable Growth Fund since 2016 and leads its healthcare efforts in the U.S. Whilst at Bridges he served on the board of directors of the following private companies, which are, or have been, investees of Bridges: Impact Fitness North America, LP (2016 to 2019); Medwood Services, LLC (chairman of the board) (2018 to present); Sunrise Treatment Center, LLC (chairman of the board) (2019 to present); Jump City Holdings, Inc (2019 to present); James River Home Health and Hospice, LLC (2020 to present) and Altius Healthcare Management, LLC (chairman of the board) (2021 to present). Prior to Bridges, Mr. Niemczyk was an investor at The Beekman Group, LLC and Cordova, Smart and Williams, LLC and started his career at GE Capital Corporation. Mr Niemczyk holds a BA from Franklin & Marshall College and an MBA from Columbia Business School.
Family Relationships
Other than Dr. Michael Leek and Ms. Angela Scott who are married, there are no family relationships among any of the members of our senior management or board of directors.
| B. | Compensation |
Compensation of Senior Management and Directors
For the year ended December 31, 2021, the aggregate compensation accrued or paid to the members of our board of directors and our senior management for services in all capacities, including defined contribution pensions and share-based compensation, was £1.05 million. As at December 31, 2021, the board of directors and our senior management held share options over 2,529,560 ordinary shares.
Senior Management Employment Arrangements and Service Agreements
We have entered into employment agreements with certain of our senior management persons. These agreements generally provide for a base salary, an annual cash bonus, and share option grants as the form of compensation. The agreements also provide for the following benefits: pension contributions, health insurance and group life insurance.
Non-Executive Director Appointment Letters
The compensation of our non-executive directors is determined by our board of directors as a whole, based, in part, on a review of current practices in other companies. We enter into a letter agreement with each director stating their compensation arrangement.
Equity Compensation Plans
We have two share option schemes for future grants to directors, employees and consultants. Notwithstanding the terms of the plans as set forth below, award grants to consultants in any one year are limited to not more than 1,000,000 ordinary shares pursuant to the terms of the public Warrants. Details of the share option schemes are summarized below.
2014 Share Option Scheme (as amended)
On December 16, 2014, we adopted a share option scheme, or the 2014 Share Option Scheme, for the purpose of enabling the grant of share options to incentivize our employees and employees of our subsidiary companies.
The 2014 Share Option Scheme permits grants of (i) enterprise management incentive (“EMI”) options which are potentially tax-advantaged in the United Kingdom under the terms of Schedule 5 to the United Kingdom Income Tax (Earnings and Pensions) Act 2003 (subject to the relevant conditions being met by the company and the grantee) and (ii) “unapproved” options (which do not attract tax advantages as they have not been “approved” by the U.K. tax authority, HMRC).
As of December 31, 2021, we had granted options to purchase 5,329,230 ordinary shares under the 2014 Share Option Scheme and no further awards are expected to be granted. All of these options have vested.
| 109 |
Class of Share: An option granted under the 2014 Share Option Scheme entitles the option holder, subject to the satisfaction, waiver or acceleration of specific exercise conditions, to subscribe for O ordinary shares. All options granted under the 2014 Share Option Scheme over O ordinary shares have been exchanged for equivalent options over ordinary shares as a result of the corporate reorganization of the Company. Subject to minor amendments, all material terms of the Options will remain the same as prior to the exchange.
Exercise Condition: Options granted under our 2014 Share Option Scheme may be granted subject to vesting schedules, performance targets or other conditions which must be satisfied or waived before exercise. Exercise conditions may be removed or varied by our board of directors, provided that any variation shall be (in the reasonable opinion of our board of directors) no more difficult to satisfy than the original exercise condition (unless otherwise approved by grantees).
Option Agreements: Each option grant is documented through an option agreement. Most of the option agreements entered into under the 2014 Share Option Scheme provide that all unexercised options are exercisable upon one or more of the following events: (i) the admission of any of the Company’s ordinary shares (a) to the Official List of the UK Listing Authority and to trading on the London Stock Exchange’s market for listed securities, or (b) to trading on the Alternative Investment Market of the London Stock Exchange or (c) to listing on a “recognized stock exchange” within the meaning of sections 1005(3) and 1005(4) of the Income Tax Act 2007 (ITA 2007) (which includes Nasdaq); (ii) a sale of 90% of the business or undertakings of the Company; and (iii) the acquisition by a third party of 90% or more of the issued share capital of the Company.
Leaver Provision:. If an option holder is subject to a formal disciplinary procedure, their option will lapse. In other instances of cessation of employment, the board will determine, within 90 days, whether to permit exercise or lapse of the Options belonging to that leaver.
Lapse of Option:. If not otherwise lapsed in accordance with the provisions of the 2014 Share Option Scheme, an option granted under the 2014 Share Option Scheme shall lapse on the day before the 10th anniversary of the grant of the option.
If an option holder dies, his or her personal representatives may exercise his or her options within a period ending on the earlier of (i) the expiry of 12 months after the date of death, and (ii) the day before the 10th anniversary of the grant of the option, only to the extent that any exercise conditions have been met (unless waived by the board). Failing such exercise, the deceased option holder’s options shall lapse.
Adjustment of Award:. In the event that there is any variation in our share capital that affects the value of the options, our board of directors will make such adjustments to the number and exercise price of shares subject to each option or the option price as our board of directors considers appropriate in accordance with the rules of the 2014 Share Option Scheme.
Transferability: No options under the 2014 Share Option Scheme may be transferred, assigned or have any created over them and will lapse immediately upon an attempt to do so (other than an assignment to personal representatives upon death).
Amendment: Our board of directors may, amend the 2014 Share Option Scheme, provided that any amendment shall not, without the consent of an option holder, materially increase his or her liabilities or materially decrease the value of his or her subsisting rights under an outstanding option.
The rules of the 2014 Share Option Scheme have been amended such that any amendment to the scheme shall take effect at the discretion of the board of directors, except as otherwise required by applicable laws or the rules of any securities exchange on which our securities are listed.
2021 Share Option Scheme
The Board of directors adopted on January 12, 2022, a share option scheme, or the 2021 Share Option Scheme, for the purpose granting share options to incentivize our directors, employees and consultants and the directors, employees and consultants of our subsidiary companies. The 2021 Share Option Scheme incorporates a sub-plan for option holders subject to taxation in the United States, or the 2021 U.S. Sub-Plan, to provide for the grant of U.S. qualified incentive options.
| 110 |
The 2021 Share Option Scheme permits grants of (i) enterprise management incentive options which are potentially tax-advantaged in the United Kingdom under the terms of Schedule 5 to ITEPA 2003 (subject to the relevant conditions being met by the company and the grantee); (ii) “unapproved” options (which do not attract tax advantages as they have not been “approved” by the U.K. tax authority, HMRC); and (iii) incentive stock options (“ISO”) and non-qualified stock options under the 2021 U.S. Sub-Plan for US resident grantees.
The board of directors may grant such awards under the 2021 Share Option Scheme as it may determine at its discretion, provided always that adequate share capital is available to enable the exercise of all options so granted.
As of December 31, 2021, there were no options granted under the 2021 Shares Option Scheme. Since the year end, however, immediately after the February 2022 IPO, we granted options to purchase 2,583,491 ordinary shares at an exercise price of $4.25, under the 2021 Share Option Scheme of which 831,081 are vested.
Class of Share: An option granted under the 2021 Share Option Scheme entitles the option holder, subject to the satisfaction, waiver or acceleration of specific exercise conditions, to subscribe for ordinary shares.
Exercise Conditions: Options granted under our 2021 Share Option Scheme may be granted subject to vesting schedules, performance targets or other conditions which must be satisfied or waived before exercise. Exercise conditions may be removed or varied by our board of directors, provided that any variation shall be (in the reasonable opinion of our board of directors) no more difficult to satisfy than the original exercise condition. The board may also at its discretion impose a further “lock-in period”, following vesting, during which options cannot be exercised.
Each option grant is documented through an option certificate. Upon the occurrence of a takeover or certain similar corporate events, the option will be exercisable to the extent vested, though the board will have authority to permit an immediate vesting immediately prior to the relevant event.
Leaver Provisions: If an option holder ceases to be an employee or director of the company or a subsidiary and is a good leaver (broadly an option holder who leaves other than for cause, as defined in the plan rules), the option holder may exercise his options during the three years after the date of such cessation of employment/directorship (unless the board varies this period) only to the extent vested and that any exercise conditions have been met at the time of such cessation of employment/directorship, although the board may exercise its discretion to accelerate vesting and/or waive any exercise conditions. Any part of an option which is not exercisable shall lapse. If EMI Options or ISO options are retained for more than 90 days following a cessation of employment, they will cease to qualify for relevant tax benefits. Any option holder who leaves and is not a good leaver will lose their options entirely, regardless of vesting.
Lapse of Options: If not otherwise lapsed in accordance with the provisions of the 2021 Share Option Scheme, an option granted under the 2021 Share Option Scheme shall lapse on the 10th anniversary of the grant of the option. Option shares subject to lapsed option grants will be available to be re-granted under new option grants. If an option holder dies, his or her personal representatives may exercise his or her options within a period ending on the earlier of (i) the expiry of 12 months after the date of death, and (ii) the 10th anniversary of the grant of the option, only to the extent vested at the time of death (unless the board agrees to waive any exercise conditions or accelerate vesting). Failing such exercise, the deceased option holder’s options shall lapse.
Adjustment of Award: In the event that there is any variation in our share capital that affects the value of the options, our board of directors will make such adjustments to the number and exercise price of shares subject to each option or the option price as our board of directors considers appropriate in accordance with the rules of the 2021 Share Option Scheme.
Takeovers and Corporate Events: If (a) any person or group of persons acting in concert obtains control (meaning more than 50% of the voting rights) of the company, (b) there is a disposal of all or substantially all of the assets of the group to a third party; or (c) the Company is wound up, an option holder may at any time exercise his or her vested options or any part thereof which has not lapsed within a specified period and the board may exercise its discretion to accelerate vesting or waive exercise conditions. To the extent they are not exercised, such options will lapse at the end of the specified period for exercise.
| 111 |
Transferability: No options under the 2021 Share Option Scheme may be transferred, assigned or have any created over them (other than in the case of an assignment to personal representatives upon death) and will lapse immediately upon an attempt to do so.
Amendment: Our board of directors may amend the 2021 Share Option Scheme in non-material ways, provided that any amendment shall not, without the consent of an option holder, materially increase his or her liabilities or materially decrease the value of his or her subsisting rights under an outstanding option. Material changes to the 2021 Share Option Scheme will require shareholder approval.
2021 U.S. Sub-Plan
The 2021 U.S. Sub-Plan applies to grantees that are subject to U.S. federal income tax and governs only those grants that are intended to be incentive stock options (“ISO”) pursuant to Section 422 of the Internal Revenue Code. All options granted to U.S persons will be granted at not less than 100% of the fair market value of an underlying shares on the date of grant, and certain incentive stock options will have to be granted at 110% of fair market value of an underlying share on the date of grant. All stock options issued to U.S persons that are not exercised within 10 years from the grant date expire, provided that incentive stock options granted to a person holding more than 10% of our voting power will expire within five years from the date of grant. With respect to grantees that are subject to U.S. federal income tax, the 2021 Share Option Scheme, the 2021 U.S. Sub-Plan and all options issued thereunder are intended to comply with, or be exempt from, Section 409A of the Internal Revenue Code, and they are to be interpreted accordingly. In the event that any option is subject to Section 409A of the Internal Revenue Code, our board of directors, in their sole discretion, may amend the 2021 Share Option Scheme, the 2021 U.S. Sub-Plan and any option issued thereunder, adopt policies and procedures or take such other actions as our board of directors deems appropriate, to exempt the 2021 Share Option Scheme, the 2021 U.S. Sub-Plan or any option from Section 409A of the Internal Revenue Code, to preserve the intended tax treatment of such option or comply with the requirements of Section 409A of the Internal Revenue Code.
2021 Company Share Option Plan (2021 CSOP)
The Board of Directors approved a share option scheme, or the 2021 CSOP, for the purpose of enabling the grant of share options to incentivize our employees and employees of our subsidiary companies.
The 2021 CSOP is an option scheme that provides for the grant of options which affords some tax advantages to the option holder who are UK taxpayers, where the tax benefits afforded under the EMI option scheme rules no longer qualify. While the CSOP scheme is broadly similar in terms of its tax advantages it is more limited in terms of the quantum of the award (EMI options may be granted over shares worth up to £250,000 at the date of grant and for CSOP that number is £30,000). Grants under the CSOP would only be applicable to UK taxpayers.
Key points:
| ● | CSOP options must only be granted to full-time directors or employees; | |
| ● | each recipient can receive options to buy company shares worth up to £30,000 (as valued (ignoring any restrictions) at the date of grant or such earlier agreed time); | |
| ● | on grant of the CSOP option, there is generally no liability to income tax or NICs (employee’s and employer’s) unless the exercise price (together with any grant price) is less than the market value of the shares at the date of grant; | |
| ● | no income tax or NICs will be payable on the exercise of a tax advantaged CSOP option if the CSOP option is exercised whilst the scheme is still a tax advantaged scheme and the option is exercised; |
| 112 |
| ○ | on or before the tenth anniversary of the date of grant of the option, and either; | |
| ○ | on or after the third anniversary of the date of grant; or | |
| ○ | pursuant to the terms of the CSOP, prior to the third anniversary of the date of grant and, broadly, within six months of certain takeover events and/or certain “good leaver” events; |
| ● | there is no capital gains tax (CGT) payable on the grant or exercise of a qualifying CSOP option. On sale of the option shares, CGT may be payable on any gain; | |
| ● | the CSOP scheme rules include the concept of a vesting requirement before they can be exercised and CSOP option awards are generally structured so that they do not become exercisable/vest earlier than three years from grant so that they provide the preferential tax treatment to the option holder (the board could provide for a longer vesting period if it wished, but not shorter); | |
| ● | option awards which have not vested on an option holder’s cessation of employment lapse;
a restricted class of “good leavers” (those who leave for involuntary reasons) may exercise their vested options if they leave within the first three years after grant. Non-good leavers will not be permitted to exercise options in the first three years after grant and their options shall lapse. After the first three years, the same rules for leavers apply as for the 2021 Share Option Scheme; and | |
| ● | the option holder indemnifies the Company in relation to Tax Liabilities (as defined in the CSOP rules) should they arise to any group company. |
To qualify for beneficial tax treatment under the EMI and CSOP codes, the exercise price of options must not be less than the market value of the underlying shares. The Company is seeking approval from HMRC that, when granting EMI and/or CSOP options, the closing price on the immediately preceding business day can be relied on as market value for these purposes.
| C. | Board Practices |
Corporate Governance Practices
We are a “foreign private issuer” under applicable federal securities laws and regulations. In accordance with Nasdaq listing requirements, we comply with home country governance requirements and certain exemptions thereunder rather than complying with Nasdaq corporate governance standards applicable to U.S. domestic listed companies. While we voluntarily follow many Nasdaq corporate governance rules, we will take advantage of the following limited exemptions:
| ● | Scottish law does not require that a majority of our board of directors consist of independent directors or that our board committees consist of entirely independent directors. Our board of directors and board committees, therefore, may include fewer independent directors than would be required if we were subject to Nasdaq Listing Rule 5605(b)(1). In addition, we will not be subject to Nasdaq Listing Rule 5605(b)(2), which requires that independent directors must regularly have scheduled meetings at which only independent directors are present. | |
| ● | Exemption from the requirement to have a nominations committee of the board of directors. | |
| ● | Exemption from quorum requirements applicable to meetings of shareholders. Such quorum requirements as established by Nasdaq are generally not required under Scottish law. In accordance with generally accepted business practice, our Articles of Association will provide alternative quorum requirements that are generally applicable to meetings of shareholders. |
| 113 |
| ● | Exemption from the Nasdaq rules applicable to domestic issuers requiring disclosure within four business days of any determination to grant a waiver of the code of business conduct and ethics to directors and officers. Although we will require board approval of any such waiver, we may choose to disclose waivers by any of the following means: providing website disclosure that satisfies the requirements of Item 5.05I of Form 8-K; including disclosure in a Form 6-K or in the next Form 20-F; or by distributing a press release. | |
| ● | Exemption from the requirement to obtain shareholder approval for certain issuances of securities, including (i) the acquisition of the stock or assets of another company; (ii) equity-based compensation of officers, directors, employees or consultants; (iii) a change of control of the Company; and (iv) certain transactions such as private placements of the Company’s securities. |
We follow the practices of our home country, Scotland, in lieu of the foregoing requirements. Although we may rely on home country corporate governance practices in lieu of certain of the rules in the Nasdaq Rule 5600 Series and Rule 5250(d), we must comply with Nasdaq’s Notification of Noncompliance requirement (Rule 5625) and the Voting Rights requirement (Rule 5640). Further, we must have an audit committee that satisfies Nasdaq Rule 5605(c)(3), which addresses audit committee responsibilities and authority and requires that the audit committee consist of members who meet the independence requirements of Nasdaq Rule 5605(c)(2)(A)(ii).
Although we currently intend to comply with the Nasdaq corporate governance rules applicable other than as noted above, we may in the future decide to use the foreign private issuer exemption with respect to some or all the other Nasdaq corporate governance rules.
In addition, as a foreign private issuer, we will not be subject to certain SEC reporting obligations:
| ● | Filing quarterly reports on Form 10-Q or provide current reports on Form 8-K disclosing significant events within four days of their occurrence; | |
| ● | The rules and regulations governing proxy solicitations of the SEC; | |
| ● | Certain requirements of Regulation FD, which governs certain disclosure obligations of a reporting company which may be selective; and | |
| ● | Our officers, directors and 10% and greater stockholders will be exempt from Section 16 rules regarding purchases and sales of our securities, which will provide less data in this regard than shareholders of U.S. companies that are subject to the Exchange Act. |
Accordingly, our shareholders do not have the same protections afforded to shareholders of companies that are subject to all of the corporate governance requirements of Nasdaq and the domestic reporting requirements of the SEC. We may utilize these exemptions for as long as we continue to qualify as a foreign private issuer.
Composition of Our Board of Directors
Our board of directors is currently composed of seven members. As a foreign private issuer, under the listing requirements and rules of Nasdaq, we are not required to have independent directors on our board of directors, except that our audit committee is required to consist fully of independent directors, subject to certain phase-in schedules. Notwithstanding the Nasdaq listing requirements, our board of directors has determined that Dr Mark Bonyhadi, James Culverwell, Arlene Morris and Edward Niemczyk, representing a majority (four) of the seven directors, do not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of director and that each of these directors is “independent” as that term is defined under Nasdaq rules.
Directors’ service contracts include notice periods of between six and twelve months. The service contracts do not include terms that provide for benefits payable upon termination, other than in regard to payment in lieu of notice in appropriate.
| 114 |
Committees of Our Board of Directors
Our board of directors has two standing committees: an audit committee and a remuneration committee.
Audit Committee
The audit committee consists of James Culverwell (chair), Arlene Morris and Edward Niemczyk. It assists the board of directors in overseeing our accounting and financial reporting processes. The audit committee consists exclusively of members of our board who are financially literate, and our board of directors has determined that James Culverwell is an “audit committee financial expert” as defined by applicable SEC rules and has the requisite financial sophistication as defined under the applicable Nasdaq rules and regulations. Our board of directors has determined that each member of the audit committee is an independent director under Nasdaq listing rules and under Rule 10A-3 under the Exchange Act. Our audit committee meets regularly each year and oversee and review our internal controls, accounting policies and financial reporting, and provide a forum through which our independent registered public accounting firm reports. Our audit committee also meets regularly with our independent registered public accounting firm without management present. The audit committee is governed by a charter that complies with Nasdaq rules.
The audit committee’s responsibilities include:
| ● | recommending the appointment of the independent auditor to shareholders for approval at the general meeting of shareholders; | |
| ● | the appointment, compensation, retention and oversight of any accounting firm engaged for the purpose of preparing or issuing an audit report or performing other audit services; | |
| ● | pre-approving the audit services and non-audit services to be provided by our independent auditor before the auditor is engaged to render such services; | |
| ● | evaluating the independent auditor’s qualifications, performance, and independence, and presenting its conclusions to the full board of directors on at least an annual basis; | |
| ● | reviewing and discussing with management and our independent registered public accounting firm our financial statements and our financial reporting process; and | |
| ● | reviewing, approving, or ratifying any related party transactions. |
Remuneration Committee
The remuneration committee consists of Arlene Morris (chair), James Culverwell and Edward Niemczyk. Under SEC and Nasdaq rules, there are heightened independence standards for members of the remuneration committee, including a prohibition against the receipt of any compensation from us other than standard board member fees. The remuneration committee is governed by a charter that complies with Nasdaq rules. Although foreign private issuers are not required to meet this heightened standard, all of our remuneration committee members are expected to meet this heightened standard.
The remuneration committee’s responsibilities include:
| ● | identifying, reviewing and proposing policies relevant to the compensation and benefits of our directors and senior management; | |
| ● | evaluating the performance of senior management in light of such policies and reporting to the board; and | |
| ● | overseeing and administering our employee share option scheme or equity incentive plans in operation from time to time. |
Code of Business Conduct and Ethics
We have adopted a Code of Business Conduct and Ethics, or Code of Ethics, applicable to our employees, senior management, and directors, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. A current copy of the Code of Ethics is posted on our website, which is located at www.tcbiopharm.com. Information contained on, or that can be accessed through, our website does not constitute a part of this Annual Report and is not incorporated by reference herein.
| 115 |
Insurance and Indemnification
To the extent permitted by the Companies Act 2006 (the Companies Act), we are empowered to indemnify our directors against any liability they incur by reason of their directorship. We maintain directors’ and officers’ insurance to insure such persons against certain liabilities. We have entered into a deed of indemnity with each of our directors and members of our senior management.
Insofar as indemnification of liabilities arising under the United States securities laws may be permitted to our board of directors, senior management, or persons controlling us pursuant to the foregoing provisions, we have been informed that, in the opinion of the SEC, such indemnification is against public policy and is therefore unenforceable.
| D. | Employees |
We have 76 full-time equivalent employees. Of these employees, 60 were in research and development (including in manufacturing and operations, and quality control and quality assurance), 10 in other key functions (including clinical, business development, finance, intellectual property, information technology and general administration) and 4 members of the executive team. We have never had a work stoppage and none of our employees are covered by collective bargaining agreements or represented by a labor union. We believe our employee relations are good.
At each date shown, we had the following number of employees engaged in either administrative or research and development functions, as indicated below.
| At December 31, | ||||||||||||
| 2019 | 2020 | 2021 | ||||||||||
| Function: | ||||||||||||
| Administrative | 11 | 13 | 8 | |||||||||
| Research and development | 83 | 66 | 68 | |||||||||
| Total | 94 | 79 | 76 | |||||||||
| Geography: | ||||||||||||
| United Kingdom | 94 | 79 | 75 | |||||||||
| United States of America | - | - | 1 | |||||||||
Our human capital resources objectives include, as applicable, identifying, recruiting, retaining, incentivizing and integrating our existing and additional employees. The principal purposes of our equity incentive plans are to attract, retain and motivate selected employees, consultants and directors through the granting of equity-based compensation awards.
| E. | Share Ownership. |
For information regarding the share ownership of our directors and executive officers, see “Item 7.A—Major Shareholders.”
| Item 7. | Major Shareholders and Related Party Transactions |
| A. | Major Shareholders |
The following table and related footnotes set forth information with respect to the beneficial ownership of our ordinary shares as of March 1, 2022 by:
| ● | each of our executive officers and directors; |
| 116 |
| ● | each person beneficially owning more than 5% of our share capital; and | |
| ● | all executive officers and directors as a group. |
Beneficial ownership, unless otherwise noted is derived from company records, and is based upon 28,063,909 ordinary shares issued and outstanding on March 1, 2022, which number includes those represented in the trading market by ADSs. In computing the number of ordinary shares owned by a person and the percentage ownership of that person, as determined in accordance with the rules and regulations of the SEC, we have included shares that the person has the right to acquire within 60 days from March 1, 2022, including through the exercise of any option, warrant or other right or the conversion of any other security. All major shareholders have the same voting rights.
Unless otherwise noted below, each beneficial owner’s address is: c/o Maxim 1, 2 Parklands Way, Holytown, Motherwell, ML1 4WR, Scotland, United Kingdom.
| No. of Ordinary Shares Beneficially Owned | Percentage Owned | |||||||
| Holders of more than 5% of our voting securities: | ||||||||
| Entities affiliated with Renaissance Capital Partners Limited (1) | 9,225,412 | 27.6 | % | |||||
| Scottish Enterprise (2) | 4,432,683 | 15.8 | % | |||||
| MEDINET Co., Ltd (3) | 3,675,000 | 13.1 | % | |||||
| Dr. Michael Leek (4) (*) | 2,235,876 | 7.5 | % | |||||
| Angela Scott (5) | 2,044,746 | 7.0 | % | |||||
| NIPRO Corporation (6) | 1,930,500 | 6.9 | % | |||||
| Alta Partners LLC (7) | 1,866,342 | 6.4 | % | |||||
| Directors and executive officers who are not 5% holders: | ||||||||
| Bryan Kobel (8) (*) | 105,060 | 0.4 | % | |||||
| Martin Thorp (9) (*) | 496,136 | 1.7 | % | |||||
| Dr. Mark Bonyhadi (10) (*) | - | 0.0 | % | |||||
| James Culverwell (11) (*) | - | 0.0 | % | |||||
| Arlene Morris (12) (*) | - | 0.0 | % | |||||
| Edward Niemczyk (13) (*) | - | 0.0 | % | |||||
| All directors and officers as a group (14) | 4,881,818 | 15.8 | % | |||||
| Total | ||||||||
(*) Indicates a director of TC BioPharm (Holdings) plc.
(1) Two directors of Renaissance Capital Partners Limited (including Mark Randall, Kenneth Randall and Diane Randall) are also shareholders in TC BioPharm (Holdings) plc and for the purposes of this table Renaissance Capital Partners Limited is deemed to be the beneficial owner of those securities. The beneficial interest of the affiliated entities consists of (a) 3,918,948 issued ordinary shares, and (b) and 5,306,464 ordinary shares underlying public Warrants. This information was determined by reference to a Schedule 13D filed by Renaissance Capital Partners Limited on April 27, 2022.
(2) The address of Scottish Enterprise, an agency of the Scottish government, is Atrium Court, 50 Waterloo Street, Glasgow, G2 6HQ. The board of directors of the stockholder exercises the voting and dispositive authority over the shares held by this stockholder.
(3) The address of Medinet Co., Ltd. is TRC Center Bldg. 9F, 6-1-1 Heiwajima, Ota-ku, Tokyo, 143-0006 JAPAN. The board of directors of the stockholder exercises the voting and dispositive authority over the shares held by this stockholder.
(4) Consists of (a) 664,220 issued ordinary shares and (b) 1,571,656 ordinary shares that are immediately exercisable within 60 days of the above date, but does not include 561,196 ordinary shares that may be acquired under outstanding options and/or warrants 60 days after the above date. Ms Scott is the spouse of Dr. Michael Leek, however, her financial affairs historically have been handled separately from those of Dr. Leek, and therefore her shareholding is not combined for purposes of this table.
| 117 |
(5) Consists of (a) 741,310 issued ordinary shares and (b) 1,303,436 ordinary shares that are exercisable within 60 days of the above date, but does not include 561,196 ordinary shares that may be acquired 60 days after the above date. Dr. Leek is the spouse of Ms. Angela Scott, however, his financial affairs historically have been handled separately from those of Ms. Scott, and therefore his shareholding is not combined for purposes of this table.
(6) The address of NIPRO Corporation is 3-9-3, Honjo-Nishi, Kita-ku, Osaka 531-8510, Japan. The board of directors of the stockholder exercises the voting and dispositive authority over the shares held by this stockholder.
(7) The address of Alta Partners LLC is 954 Avenida Ponce de Leon, Suite 207, San Juan PR 00907. The board of directors of the stockholder exercises the voting and dispositive authority over the shares held by this stockholder. The beneficial interests of the stockholder consist of (a) 909,960 issued ordinary shares and (b) 956,382 ordinary shares underlying public Warrants. This information was determined by reference to a Schedule 13G filed by Alta Partners LLC on March 17, 2022.
(8) Bryan Kobel beneficially owns 105,060 ordinary shares owned by TCB-AFOS I LLC over which Mr. Kobel has voting and dispositive authority as the manager, but as to which Mr. Kobel disclaims any other beneficial ownership interest as he is not a member of the LLC.
(9) Consists of (a) Nil ordinary shares and (b) 496,136 ordinary shares that are exercisable within 60 days of the above date, but does not include 561,196 ordinary shares that may be acquired 60 days after the above date.
(10) Does not include 22,500 ordinary shares that may be acquired 60 days after the above date.
(11) Does not include 22,500 ordinary shares that may be acquired 60 days after the above date.
(12) Does not include 22,500 ordinary shares that may be acquired 60 days after the above date.
(13) Does not include 22,500 ordinary shares that may be acquired 60 days after the above date.
(14) Consists of (a) 1,510,590 ordinary shares and (b) 3,371,228 ordinary shares that are exercisable within 60 days of the above date, but does not include 1,773,588 ordinary shares that may be acquired 60 days after the above date.
As of March 1, 2022, assuming that all of our ordinary shares represented by ADSs are held by residents of the United States other than ADSs held by the entities set forth in the table above and certain other holders that we know to be non-residents of the United States, we estimate that approximately 16% of our outstanding ordinary shares (including ordinary shares underlying ADSs) were held in the United States by 4 holders of record.
As of March 1, 2022, assuming that all of our Warrants are held by residents of the United States other than Warrants held by the entities set forth in the table above and certain other holders that we know to be non-residents of the United States, we estimate that approximately 62% of our Warrants were held in the United States by 4 holders of record.
The actual number of holders is greater than these numbers of record holders, and includes beneficial owners whose ordinary shares are held in street name by brokers and other nominees. This number of holders of record also does not include holders whose shares may be held in trust by other entities.
| B. | Related Party Transactions |
The following is a description of related party transactions we have entered into since January 1, 2020, with any members of our board of directors, executive officers or the holders of more than 5% of our share capital.
During the years ended December 31, 2020 and 2021, the Group made purchases of cell culture media from Cell Science & Technology Institute, Inc., a company in which significant shareholder NIPRO Corporation (Osaka, Japan), has a significant interest in the amount of £30,775 and £52,795 respectively.
During the years ended December 31, 2020 and 2021, the Group used consultancy services from Theraldia Consulting Limited a company in which Dr Alan Clark has a significant interest in the amount of £22,621 and £Nil respectively.
During the year ended December 31, 2020, the executive directors agreed to defer a proportion of their compensation. Repayment of deferred compensation would be initiated on receipt of an agreed level of funding to support the future capital requirements of the business and settlement would be staged over twelve months. As at December 31, 2021 the balance outstanding to executive directors totaled £591,886 (2020: £253,338).
| 118 |
Bryan Kobel beneficially owns 105,060 shares of the Company owned by TCB-AFOS I LLC over which Mr. Kobel has voting and dispositive authority as the manager, but as to which Mr. Kobel disclaims any other beneficial ownership interest as he is not a member of the LLC.
Subscriptions in our A Ordinary shares
On August 25, 2020, we issued and sold 348,830 A ordinary shares to Scottish Enterprise, an agency of the Scottish government and a shareholder with more than 5% of our share capital.
On April 30, 2021, we issued and sold 23,260 A ordinary shares to Renaissance Capital Partners Limited, a shareholder with more than 5% of our share capital.
Immediately prior to the IPO, under the terms of our Articles of Association to certain shareholders who, prior to the IPO, owned certain ordinary share which carried the right, are eligible to subscribe at nominal value for a certain number of additional shares, calculated by reference to the pre-money valuation of the IPO. As part of this issue Scottish Enterprise are eligible to acquire an additional 248,290 ordinary shares and Renaissance Capital Partners Limited are eligible to acquire an additional 16,560 ordinary shares.
Issuance of Convertible Loan Notes
On April 30, 2021, we issued Convertible Loan Notes with a face value of $2,768,000 for a cash subscription value of $1,384,000 to Renaissance Capital Partners Limited, a shareholder with more than 5% of our share capital. On June 24, 2021, we issued Convertible Loan Notes with a face value of $1,395,700 for a cash subscription value of $697,850 to Renaissance Capital Partners Limited, a shareholder with more than 5% of our share capital. On July 28, 2021, we issued Convertible Loan Notes with a face value of $2,754,928 for a cash subscription value of $1,377,464 to Renaissance Capital Partners Limited, a shareholder with more than 5% of our share capital. On September 21, 2021, we issued Convertible Loan Notes with a face value of $1,000,000 for a cash subscription value of $500,000 to Sixth Borough Capital Fund, LP, a shareholder with more than 5% of our share capital. On October 7, 2021, we issued Convertible Loan Notes with a face value of $2,000,000 for a cash subscription value of $1,000,000 to Alta Partners LLC, a shareholder with more than 5% of our share capital. On October 18, 2021, we issued Convertible Loan Notes with a face value of $2,000,000 for a cash subscription value of $1,000,000 to Sixth Borough Capital Fund, LP, a shareholder with more than 5% of our share capital. On December 24, 2021, we issued Convertible Loan Notes with a face value of $1,620,000 for a cash subscription value of $750,000 to Renaissance Capital Partners Limited, a shareholder with more than 5% of our share capital. On December 30, 2021, we issued Convertible Loan Notes with a face value of $1,000,000 for a cash subscription value of $500,000 to Alta Partners LLC, a shareholder with more than 5% of our share capital.
Registration Rights
The Company granted the holders of the Convertible Loan Notes a limited registration right to register for resale the ordinary shares (or ADSs if the ordinary shares are dematerialized) for resale. The Company registered the ADSs and Warrants issued upon the conversion of the notes that occurred in connection with the February 2022 IPO and thereafter the two succeeding conversion dates.
| C. | Interests of Experts and Counsel |
Not Applicable
| Item 8 | Financial Information |
| A. | Consolidated Statements and Other Financial Information |
See “Item 18. Financial Statements.”
| 119 |
Dividend Policy
We have never declared or paid a dividend, and we do not anticipate declaring or paying dividends in the foreseeable future. We intend to retain all available funds and any future earnings to fund the development and expansion of our business.
Under English law, among other things, we may only pay dividends if we have sufficient distributable reserves (on a non-consolidated basis), which are our accumulated realized profits that have not been previously distributed or capitalized less our accumulated realized losses, so far as such losses have not been previously written off in a reduction or reorganization of capital.
| B. | Significant Changes |
Not applicable
| Item 9. | The Offering and Listing |
| A. | Offering and Listing Details |
The ADSs and public Warrants have been listed on the Nasdaq Capital Market under the symbols “TCBP” and “TCBPW,” respectively, since February 11, 2022.
| B. | Plan of Distribution |
Not applicable
| C. | Markets |
The ADSs and public Warrants have been listed on the Nasdaq Capital Market under the symbols “TCBP” and “TCBPW,” respectively, since February 11, 2022.
| D. | Selling Shareholders |
Not applicable
| E. | Dilution |
Not applicable
| F | Expenses of the Issuer |
Not applicable
| Item 10. | Additional Information |
| A. | Share Capital |
Not applicable
| B | Memorandum and Articles of Association |
The following describes our issued share capital, summarizes the material provisions of our articles of association and highlights certain differences in corporate law in Scotland and the United States of TC BioPharm (Holdings) plc. This summary is not intended to be exhaustive. For further information, please refer to the full version of our articles of association, which are filed as an exhibit to our SEC filings.
| 120 |
Purpose
The Articles of Association contain no specific restrictions on our purpose and therefore, by virtue of section 31(1) of the Companies Act, our purpose is unrestricted.
Share Capital
Our share capital currently consists of ordinary shares. We may issue shares with such rights or restrictions as may be determined by ordinary resolution, including shares which are to be redeemed, or are liable to be redeemed at our option or the option of the holder of such shares.
Voting
The shareholders have the right to receive notice, in accordance with the Companies Act (generally 21 days), of, and to vote at, our general meetings. Each shareholder who is present in person (or, being a corporation, by representative) at a general meeting on a show of hands has one vote and, on a poll, every such holder who is present in person (or, being a corporation, by representative) or by proxy has one vote in respect of every share held by him. Generally, any resolution put to the vote of a general meeting shall be decided on a show of hands, although a poll may be demanded at the meeting on any resolution by the chairman, or by not less than five shareholders (present in person or by proxy) who are entitled to vote on the resolution, or by a shareholder or shareholders (present in person or by proxy) representing in aggregate not less than one-tenth of the total voting rights or sums paid up of all the shareholders having the right to vote on the resolution.
Variation of Rights
Whenever our share capital is divided into different classes of shares, the special rights attached to any class may be varied or abrogated either with the consent in writing of the holders of three-fourths in nominal value of the issued shares of that class or with the sanction of a special resolution (which requires a 75% vote) passed at a general meeting of the holders of the shares of that class, and may be so varied and abrogated while the company is a going concern.
Dividends
We may, subject to the provisions of the Companies Act and the Articles of Association, by ordinary resolution declare dividends to be paid to shareholders not exceeding the amount recommended by our board of directors. Subject to the provisions of the Companies Act, if, at the discretion of board of directors, our profits available for distribution justify such payments, the board of directors may pay interim dividends on any class of our share.
Any dividend unclaimed after a period of 12 years from the date such dividend was declared or became payable shall, if the board of directors’ resolve, be forfeited and shall revert to us. No dividend or other moneys payable on or in respect of a share shall bear interest as against us.
Transfer of Ordinary Shares
Each member may transfer all or any of his shares which are in certificated form by means of an instrument of transfer in any usual form or in any other form which the board of directors may approve.
The board of directors may, in its absolute discretion, refuse to register a transfer of certificated shares unless:
| (i) | it is for a share which is fully paid up; | |
| (ii) | it is for a share upon which the company has no lien; | |
| (iii) | it is only for one class of share; | |
| (iv) | it is in favor of a single transferee or no more than four joint transferees; |
| 121 |
| (v) | it is duly stamped or is duly certificated or otherwise shown to the satisfaction of the board of directors to be exempt from stamp duty; and | |
| (vi) | it is delivered for registration to the registered office of the company (or such other place as the board of directors may determine), accompanied (except in the case of a transfer by a person to whom the company is not required by law to issue a certificate and to whom a certificate has not been issued or in the case of a renunciation) by the certificate for the shares to which it relates and such other evidence as the board of directors may reasonably require to prove the title of the transferor (or person renouncing) and the due execution of the transfer or renunciation by him or, if the transfer or renunciation is executed by some other person on his behalf, the authority of that person to do so. |
Our board of directors shall not refuse to register any transfer of partly paid shares in respect of which ADSs are admitted to Nasdaq on the grounds that they are partly paid shares in circumstances where such refusal would prevent dealings in such shares from taking place on an open and proper basis.
Each shareholder may transfer all or any of his shares which are in uncertificated form by means of a relevant system in such manner provided for, and subject as provided in, the uncertificated securities rules and the Nasdaq rules. No provision of the Articles applies in respect of an uncertificated share to the extent that it requires or contemplates the effecting of a transfer by an instrument in writing or the production of a certificate for the share to be transferred.
Allotment of Shares and Preemption Rights
Subject to the Companies Act and to any rights attached to existing shares, any share may be issued with or have attached to it such rights and restrictions as the company may by ordinary resolution determine, or if no ordinary resolution has been passed or so far as the resolution does not make specific provision, as the board of directors may determine (including shares which are to be redeemed, or are liable to be redeemed at the option of the company or the holder of such shares).
In accordance with section 551 of the Companies Act, the board of directors may be generally and unconditionally authorized to exercise all the powers of the company to allot shares up to an aggregate nominal amount equal to the amount stated in the relevant ordinary resolution authorizing such allotment. The authorities referred to above were included in the ordinary resolutions passed on January 14, 2022.
The provisions of Section 561 of the Companies Act (which confer on shareholders rights of preemption in respect of the allotment of equity securities which are paid up in cash) apply to the company except to the extent disapplied by special resolution of the shareholders of the company. Such preemption rights have been disapplied by a special resolution passed on January 14, 2022.
Alteration of Share Capital
The company may by ordinary resolution consolidate its share capital into shares of larger nominal value than its existing shares, or cancel any shares which, at the date of the ordinary resolution, have not been taken or agreed to be taken by any person and diminish the amount of its share capital by the nominal amount of shares so canceled or sub-divide its shares, or any of them, into shares of smaller nominal value.
The company may, in accordance with the Companies Act, reduce or cancel its share capital or any capital redemption reserve or share premium account in any manner and with and subject to any conditions, authorities and consents required by law.
| 122 |
Board of Directors
Unless otherwise determined by the company by ordinary resolution, the number of directors (other than any alternate directors) shall not be less than two and no more than 11.
Subject to the Articles of Association and the Companies Act, the company may by ordinary resolution appoint a person who is willing to act as a director and the board of directors shall have power at any time to appoint any person who is willing to act as a director, in both cases either to fill a vacancy or as an addition to the existing board of directors. In addition to any power of removal conferred by the Companies Acts, the Company may by special resolution, or by ordinary resolution of which special notice has been given in accordance with section 312 of the Act, remove a Director at any time (without prejudice to a claim for damages for breach of contract or otherwise) and a director shall be removed from office if all other directors so direct.
Subject to the provisions of the Articles of Association, the board of directors may regulate their proceedings as they deem appropriate. A director may, and the secretary at the request of a director shall, call a meeting of the directors. The minimum notice required to call a meeting of the board of directors shall be 7 days, unless such notice is waived by all directors.
The quorum for a meeting of the board of directors is three (including at least one non-executive director and one executive director),
The first chairman of the board shall be the person that holds the office of executive chairman of the Company on the date that the Articles were adopted, who is Dr Michael Leek, and in the event that he is unable to attend a meeting of the Board he shall be entitled to appoint another Director to act as chairman and if he does not the directors shall appoint a chairman for the meeting.
Questions and matters requiring resolution arising at a meeting shall be decided by a majority of votes of the participating directors, with each director having one vote. In the case of an equality of votes, the chairman will have a casting vote or second vote.
The directors may establish committees of the board and appoint chairpersons and members to such committees, all as it considers appropriate and at its discretion.
Directors shall be entitled to receive such compensation as the board shall determine for their services to the company as directors, and for any other service which they undertake for the company. The directors shall also be entitled to be paid all reasonable expenses properly incurred by them in connection with their attendance at meetings of shareholders or class meetings, board of director or committee meetings or otherwise in connection with the exercise of their powers and the discharge of their responsibilities in relation to the company.
The board of directors may, in accordance with the requirements in the Articles of Association, authorize any matter proposed to them by any director which would, if not authorized, involve a director breaching his duty under the Companies Act, to avoid conflicts of interests.
A director seeking authorization in respect of such conflict shall declare to the board of directors the nature and extent of his interest in a conflict as soon as is reasonably practicable. The director shall provide the board with such details of the matter as are necessary for the board to decide how to address the conflict together with such additional information as may be requested by the board.
Any authorization by the board of directors will be effective only if:
| (i) | to the extent permitted by the Companies Act, the matter in question shall have been proposed by any director for consideration in the same way that any other matter may be proposed to the directors under the provisions of the Articles; | |
| (ii) | any requirement as to the quorum for consideration of the relevant matter is met without counting the conflicted director and any other conflicted director; and | |
| (iii) | the matter is agreed to without the conflicted director, or any other interested director, voting; or would be agreed to if the conflicted director’s and any other interested director’s vote is not counted. |
Subject to the provisions of the Companies Act, every director, secretary, or other officer of the company (other than an auditor) is entitled to be indemnified against all costs, charges, losses, damages, and liabilities incurred by him in the actual purported exercise or discharge of his duties or exercise of his powers or otherwise in relation to them.
There is no shareholding requirement for directors.
| 123 |
General Meetings
The company must convene and hold an annual general meeting every year and within 6 months of the Companies accounting reference date (which is currently set at December 31), in accordance with the Companies Act. Under the Companies Act, an annual general meeting must be called by notice of at least 21 clear days.
No business shall be transacted at any general meeting unless a quorum is present when the meeting proceeds to business, but the absence of a quorum shall not preclude the choice or appointment of a chairman of the meeting which shall not be treated as part of the business of the meeting. Two shareholders present in person or by proxy and entitled to vote shall be a quorum for all purposes.
Borrowing Powers
Subject to the Articles of Association and the Companies Act, the board of directors may exercise all of the powers of the company to:
| (a) | borrow money; | |
| (b) | indemnify and guarantee; | |
| (c) | mortgage or charge; | |
| (d) | create and issue debentures and other securities; and | |
| (e) | give security either outright or as collateral security for any debt, liability or obligation of the company or of any third party. |
Capitalization of profits
The directors may, if they are so authorized by an ordinary resolution of the shareholders, decide to capitalize any undivided profits of the company (whether or not they are available for distribution), or any sum standing to the credit of the company’s share premium account or capital redemption reserve. The directors may also, subject to the aforementioned ordinary resolution, appropriate any sum which they so decide to capitalize to the persons who would have been entitled to it if it were distributed by way of dividend and in the same proportions.
Uncertificated Shares
Subject to the uncertificated securities rules, the board of directors may permit title to shares of any class to be issued or held otherwise than by a certificate and to be transferred by means of a “relevant system” (e.g. the depositary or custodian of the ADSs) without a certificate.
The board of directors may take such steps as it sees fit in relation to the evidencing of and transfer of title to uncertificated shares, any records relating to the holding of uncertificated shares and the conversion of uncertificated shares to certificated shares, or vice versa.
The company may by notice to the holder of an uncertificated share, require that share to be converted into certificated form.
The board of directors may take such other action that the board considers appropriate to achieve the sale, transfer, disposal, forfeiture, re-allotment or surrender of an uncertified share or otherwise to enforce a lien in respect of it.
| 124 |
Other Relevant United Kingdom Laws and Regulations
Shareholder protections found in provisions under the UK City Code on Takeovers and Mergers, or the Takeover Code, will not apply if the Company’s place of central management and control is considered to be outside of the UK (or the Channel Islands or the Isle of Man).
The Takeover Code applies to all offers for companies which have their registered offices in the United Kingdom, the Channel Islands, or the Isle of Man if any of their equity share capital or other transferable securities carrying voting rights are admitted to trading on a UK regulated market or a UK multilateral trading facility or on any stock exchange in the Channel Islands or the Isle of Man.
The Takeover Code also applies to all offers for public companies and (in certain circumstances) private companies which have their registered offices in the United Kingdom, the Channel Islands or the Isle of Man which are considered by the Takeover Panel to have their place of central management and control in the United Kingdom, the Channel Islands or the Isle of Man (the “residency test”). The Company became subject to the Takeover Code as a UK resident, UK incorporated, public limited company on 10 January 2022 when the Company re-registered as a public limited company.
The residency test for the purposes of the Takeover Code will no longer be satisfied as a majority of the Company’s directors will be resident overseas. Therefore, shareholders of the Company will cease to be entitled to the benefit of the Takeover Code, including the rules regarding mandatory takeover bids (summarised below).
In the event that the residency test is satisfied at a point in the future the Takeover Code may apply to the Company in the future.
Mandatory Bid
Under the Takeover Code, where:
a. any person, together with persons acting in concert with such person, acquires, whether by a series of transactions over a period of time or not, an interest in shares which (taken together with shares in which such person is already interested, and in which persons acting in concert with such person are interested) carry 30% or more of the voting rights of a company; or
b. any person who, together with persons acting in concert with such person, is interested in shares which in the aggregate carry not less than 30% of the voting rights of a company but does not hold shares carrying more than 50% of such voting rights and such person, or any person acting in concert with such person, acquires an interest in any other shares which increases the percentage of shares carrying voting rights in which such person is interested;
such person shall, except in limited circumstances, be obliged to extend offers, on the basis set out in Rules 9.3, 9.4 and 9.5 of the Takeover Code, to the holders of any class of equity share capital, whether voting or non-voting, and also to the holders of any other class of transferable securities carrying voting rights. Offers for different classes of equity share capital must be comparable. the Takeover Panel should be consulted in advance in such cases.
(ii) an offer made under Rule 9 must, in respect of each class of share capital involved, be in cash or be accompanied by a cash alternative at not less than the highest price paid by the offeror or any person acting in concert with it for any interest in shares of that class during the 12 months prior to the announcement of that offer. The Panel should be consulted where there is more than one class of share capital involved.
(iii) under the Takeover Code, a “concert party” arises where persons acting together pursuant to an agreement or understanding (whether formal or informal and whether or not in writing) actively cooperate, through the acquisition by them of an interest in shares in a company, to obtain or consolidate control of the company. “Control” means holding, or aggregate holdings, of an interest in shares carrying 30% or more of the voting rights of the company, irrespective of whether the holding or holdings give de facto control.
Shareholders should note that the rules regarding mandatory takeover bids (summarised above) only apply to the Company when the Takeover Code applies.
| 125 |
Squeeze-out
| (i) | Under sections 979 to 982 of the Companies Act, if an offeror were to acquire, or unconditionally contract to acquire, not less than 90% in value of the ordinary shares of the company and 90% of the voting rights carried by the ordinary shares of the company, it could then compulsorily acquire the remaining 10%. It would do so by sending a notice to outstanding shareholders telling them that it will compulsorily acquire their shares, provided | |
| that no such notice may be served after the end of: (a) the period of three months beginning with the day after the last day on which the offer can be accepted; or (b) if earlier, and the offer is not one to which section 943(1) of the Companies Act applies, the period of six months beginning with the date of the offer. | ||
| (ii) | Six weeks following service of the notice, the offeror must send a copy of it to the company together with the consideration for the ordinary shares to which the notice relates, and an instrument of transfer executed on behalf of the outstanding shareholder(s) by a person appointed by the offeror. | |
| (iii) | The company will hold the consideration on trust for the outstanding shareholders. |
Sell-out
| (i) | Sections 983 to 985 of the Companies Act also give minority shareholders in the company a right to be bought out in certain circumstances by an offeror who has made a takeover offer. If a takeover offer relating to all the ordinary shares of the company is made at any time before the end of the period within which the offer could be accepted and the offeror held or had agreed to acquire not less than 90% of the ordinary shares, any holder of shares to which the offer related who had not accepted the offer could by a written communication to the offeror require it to acquire those shares. The offeror is required to give any shareholder notice of his right to be bought out within one month of that right arising. The offeror may impose a time limit on the rights of minority shareholders to be bought out, but that period cannot end less than three months after the end of the acceptance period, or, if longer a period of three months from the date of the notice. | |
| (ii) | If a shareholder exercises his rights, the offeror is bound to acquire those shares on the terms of the offer or on such other terms as may be agreed. |
Shareholder rights
Certain of the rights described above are only available to the holders of the ordinary shares, not to the holders of ADSs. For legal purposes, our shareholders are the persons who are registered as the owners of the legal title to the ordinary shares and whose names are recorded in our share register. If a person who holds ADSs wishes to exercise their rights a shareholders, they may be required to first take steps to withdraw their ADSs from the settlement system operated by the Depository Transfer Corporation, or DTC, and exchange their ADS for our ordinary shares thereby becoming the registered holder of the ordinary shares in our share register.
| 126 |
Differences in Corporate Law
Set forth below is a summary of certain differences between the provisions of the Companies Act applicable to us and, for sake of comparison, the General Corporation Law of the State of Delaware relating to shareholders’ rights and protections. This summary is not intended to be a complete discussion of the respective rights and it is qualified in its entirety by reference to Delaware law and the laws of Scotland.
| SCOTLAND | DELAWARE | |||
| Number of Directors | A public limited company must have at least two directors and the number of directors may be fixed by or in the manner provided in a company’s articles of association. | A corporation must have at least one director and the number of directors shall be fixed by or in the manner provided in the bylaws. | ||
| Removal of Directors | Shareholders may remove a director without cause by an ordinary resolution (which is passed by a simple majority of those voting in person or by proxy at a general meeting) irrespective of any provisions of any service contract the director has with the company, provided 28 clear days’ notice of the resolution has been given to the company and its shareholders. On receipt of notice of an intended resolution to remove a director, the company must forthwith send a copy of the notice to the director concerned. Certain other procedural requirements under the Companies Act must also be followed, such as allowing the director to make representations against his or her removal either at the meeting or in writing. | Any director or the entire board of directors may be removed, with or without cause, by the holders of a majority of the shares then entitled to vote at an election of directors, except (i) unless the certificate of incorporation provides otherwise, in the case of a corporation whose board of directors is classified, stockholders may effect such removal only for cause, or (ii) in the case of a corporation having cumulative voting, if less than the entire board of directors is to be removed, no director may be removed without cause if the votes cast against his removal would be sufficient to elect him if then cumulatively voted at an election of the entire board of directors, or, if there are classes of directors, at an election of the class of directors of which he is a part. | ||
| Vacancies on the Board of Directors | The procedure by which directors, other than a company’s initial directors, are appointed is generally set out in a company’s articles of association, provided that where two or more persons are appointed as directors of a public limited company by resolution of the shareholders, resolutions appointing each director must be voted on individually. | Vacancies and newly created directorships may be filled by a majority of the directors then in office (even though less than a quorum) or by a sole remaining director unless (i) otherwise provided in the certificate of incorporation or bylaws of the corporation or (ii) the certificate of incorporation directs that a particular class of stock is to elect such director, in which case a majority of the other directors elected by such class, or a sole remaining director elected by such class, will fill such vacancy. | ||
| Annual General Meeting | A public limited company must hold an annual general meeting, once a year, in the six-month period following the company’s annual accounting reference date. | The annual meeting of stockholders shall be held at such place, on such date and at such time as may be designated from time to time by the board of directors or as provided in the certificate of incorporation or by the bylaws. | ||
| General Meeting | A general meeting of the shareholders of a public limited company may be called by the directors.
Shareholders holding at least 5% of the paid-up capital of the company carrying voting rights at general meetings (excluding any paid up capital held as treasury shares) can require the directors to call a general meeting and, if the directors fail to do so within a certain period, may themselves convene a general meeting. |
Special meetings of the stockholders may be called by the board of directors or by such person or persons as may be authorized by the certificate of incorporation or by the bylaws. |
| 127 |
| Notice of General Meetings | At least 21 clear days’ notice must be given for an annual general meeting and state the general purpose of the meeting and present any resolutions to be proposed at the meeting. Subject to a company’s articles of association providing for a longer period, at least 14 clear days’ notice is required for any other general meeting of a public limited company. In addition, certain matters, such as the removal of directors or auditors, require special notice, which is 28 clear days’ notice. The shareholders of a company may in all cases consent to a shorter notice period, the proportion of shareholders’ consent required being 100% of those entitled to attend and vote in the case of an annual general meeting and, in the case of any other general meeting, a majority in number of the members having a right to attend and vote at the meeting, being a majority who together hold not less than 95% in nominal value of the shares giving a right to attend and vote at the meeting. | Unless otherwise provided in the certificate of incorporation or bylaws, written notice of any meeting of the stockholders must be given to each stockholder entitled to vote at the meeting not less than ten nor more than 60 days before the date of the meeting and shall specify the place, date, hour and purpose or purposes of the meeting. | ||
| Proxy | At any meeting of shareholders, a shareholder may designate another person to attend, speak and vote at the meeting on their behalf by proxy. | At any meeting of stockholders, a stockholder may designate another person to act for such stockholder by proxy, but no such proxy shall be voted or acted upon after three years from its date, unless the proxy provides for a longer period. A director of may not issue a proxy representing the director’s voting rights as a director. | ||
| Preemptive Rights | “Equity securities,” being (i) shares in the company other than shares that, with respect to dividends and capital, carry a right to participate only up to a specified amount in a distribution, referred to as “ordinary shares,” or (ii) rights to subscribe for, or to convert securities into, ordinary shares, proposed to be allotted for cash must be offered first to the existing equity shareholders in the company in proportion to the respective nominal value of their holdings, unless an exception applies or a special resolution to the contrary has been passed by shareholders in a general meeting or the articles of association provide otherwise in each case in accordance with the provisions of the Companies Act. | Stockholders have no preemptive rights to subscribe to additional issues of stock or to any security convertible into such stock unless, and except to the extent that, such rights are expressly provided for in the certificate of incorporation. | ||
| 128 |
| Authority to Allot | The directors of a company must not allot shares or grant rights to subscribe for or convert any security into shares unless an exception applies or an ordinary resolution to the contrary has been passed by shareholders in a general meeting or the articles of association provide otherwise, in each case in accordance with the provisions of the Companies Act. | If the corporation’s charter or certificate of incorporation so provides, the board of directors has the power to authorize the issuance of shares of capital stock. The board of directors may authorize capital stock to be issued for consideration consisting of cash, any tangible or intangible property or any benefit to the corporation or any combination thereof. It may determine the amount of such consideration by approving a formula. In the absence of actual fraud in the transaction, the judgment of the directors as to the value of such consideration is conclusive. | ||
| Liability of Directors and Officers | Any provision, whether contained in a company’s articles of association or any contract or otherwise, that purports to exempt a director of a company, to any extent, from any liability that would otherwise attach to him in connection with any negligence, default, breach of duty or breach of trust in relation to the company, is void. Any provision by which a company directly or indirectly provides an indemnity, to any extent, for a director of the company or of an associated company against any liability attaching to him in connection with any negligence, default, breach of duty or breach of trust in relation to the company of which he is a director is also void except as permitted by the Companies Act, which provides exceptions for the company to (i) purchase and maintain insurance against such liability; (ii) provide a “qualifying third party indemnity,” or an indemnity against liability incurred by the director to a person other than the company or an associated company or criminal proceedings in which he is convicted; and (iii) provide a “qualifying pension scheme indemnity,” or an indemnity against liability incurred in connection with the company’s activities as trustee of an occupational pension plan. | A corporation’s certificate of incorporation may include a provision eliminating or limiting the personal liability of a director to the corporation and its stockholders for damages arising from a breach of fiduciary duty as a director. However, no provision can limit the liability of a director for:
● any breach of the director’s duty of loyalty to the corporation or its stockholders;
● acts or omissions not in good faith or that involve intentional misconduct or a knowing violation of law;
● intentional or negligent payment of unlawful dividends or stock purchases or redemptions; or
● any transaction from which the director derives an improper personal benefit. |
| 129 |
| Voting Rights | Unless a poll is demanded by the shareholders of a company or is required by the chairman of the meeting or the company’s articles of association, shareholders shall vote on all resolutions on a show of hands. Under the Companies Act, a poll may be demanded by (i) not fewer than five shareholders having the right to vote on the resolution; (ii) any shareholder(s) representing not less than 10% of the total voting rights of all the shareholders having the right to vote on the resolution (excluding any voting rights attaching to treasury shares); or (iii) any shareholder(s) holding shares in the company conferring a right to vote on the resolution (excluding any voting rights attaching to treasury shares) being shares on which an aggregate sum has been paid up equal to not less than 10% of the total sum paid up on all the shares conferring that right. A company’s articles of association may provide more extensive rights for shareholders to call a poll.
Under the Companies Act, an ordinary resolution is passed on a show of hands if it is approved by a simple majority (more than 50%) of the votes cast by shareholders present (in person or by proxy) and |
Unless otherwise provided in the certificate of incorporation, each stockholder is entitled to one vote for each share of capital stock held by such stockholder. | ||
| entitled to vote. If a poll is demanded, an ordinary resolution is passed if it is approved by holders representing a simple majority of the total voting rights of shareholders present, in person or by proxy, who, being entitled to vote, vote on the resolution. Special resolutions require the affirmative vote of not less than 75% of the votes cast by shareholders present, in person or by proxy, at the meeting. |
| Stockholder Vote on Certain Transactions | The Companies Act provides for schemes of arrangement, which are arrangements or compromises between a company and any class of shareholders or creditors and used in certain types of reconstructions, amalgamations, capital reorganizations or takeovers. These arrangements require:
● the approval at a shareholders’ or creditors’ meeting convened by order of the court, of a majority in number of shareholders or creditors representing 75% in value of the capital held by, or debt owed to, the class of shareholders or creditors, or class thereof present and voting, either in person or by proxy; and
● the approval of the court.
|
Generally, unless the certificate of incorporation provides for the vote of a larger portion of the stock, completion of a merger, consolidation, sale, lease or exchange of all or substantially all of a corporation’s assets or dissolution requires:
● the approval of the board of directors; and
● the approval by the vote of the holders of a majority of the outstanding stock or, if the certificate of incorporation provides for more or less than one vote per share, a majority of the votes of the outstanding stock of the corporation entitled to vote on the matter.
|
| 130 |
| Standard of Conduct for Directors | A director owes various statutory and fiduciary duties to the company, including:
● to act in the way he considers, in good faith, would be most likely to promote the success of the company for the benefit of its members as a whole;
● to avoid a situation in which he has, or can have, a direct or indirect interest that conflicts, or possibly conflicts, with the interests of the company;
● to act in accordance with the company’s constitution and only exercise his powers for the purposes for which they are conferred;
● to exercise independent judgment;
● to exercise reasonable care, skill and diligence;
● not to accept benefits from a third party conferred by reason of his being a director or doing, or not doing, anything as a director; and
● to declare any interest that he has, whether directly or indirectly, in a proposed or existing transaction or arrangement with the company. |
Delaware law does not contain specific provisions setting forth the standard of conduct of a director. The scope of the fiduciary duties of directors is generally determined by the courts of the State of Delaware. In general, directors have a duty to act without self-interest, on a well-informed basis and in a manner they reasonably believe to be in the best interest of the stockholders.
Directors owe fiduciary duties of care and loyalty to the corporation and to its stockholders. The duty of care generally requires that a director acts in good faith, with the care that an ordinarily prudent person would exercise under similar circumstances. Under this duty, a director must inform himself of all material information reasonably available regarding a significant transaction. The duty of loyalty requires that a director act in a manner that the director reasonably believes to be in the best interests of the corporation. Directors must not use their corporate position for personal gain or advantage. In general, but subject to certain exceptions, actions of a director are presumed to have been made on an informed basis, in good faith and in the honest belief that the action taken was in the best interests of the corporation. However, this presumption may be rebutted by evidence of a breach of one of the fiduciary duties. Delaware courts have also imposed a heightened standard of conduct upon directors who take any action designed to defeat a threatened change in control of the corporation.
In addition, when the board of directors approves the sale or break-up of a corporation, the board of directors may, in certain circumstances, have a duty to obtain the highest value reasonably available to the stockholders. | ||
| Stockholder Litigation | Under Scottish law, generally, the company, rather than its shareholders, is the proper claimant in an action in respect of a wrong done to the company or where there is an irregularity in the company’s internal management. Notwithstanding this general position, the Companies Act provides that (i) a court may allow a shareholder to bring a derivative claim (that is, an action in respect of and on behalf of the company) in respect of a cause of action arising from a director’s negligence, default, breach of duty or breach of trust and (ii) a shareholder may bring a claim for a court order where the company’s affairs have been or are being conducted in a manner that is unfairly prejudicial to some of its shareholders. | A stockholder may initiate a derivative action to enforce a right of a corporation if the corporation fails to enforce the right itself. The complaint must:
● state that the plaintiff was a stockholder at the time of the transaction of which the plaintiff complains or that the plaintiff’s shares thereafter devolved on the plaintiff by operation of law; and
● allege with particularity the efforts made by the plaintiff to obtain the action the plaintiff desires from the directors and the reasons for the plaintiff’s failure to obtain the action; or
● state the reasons for not making the effort.
Additionally, the plaintiff must remain a stockholder through the duration of the derivative suit. The action will not be dismissed or compromised without the approval of the Delaware Court of Chancery. |
| 131 |
American depositary shares
The Bank of New York Mellon acts as the depositary for the ADSs. As depositary, The Bank of New York Mellon will register and deliver the ADSs. Each ADS represents one ordinary share (or a right to receive and to exercise the beneficial ownership interests in one ordinary share) deposited with The Bank of New York Mellon, or any successor, as custodian, acting through an office located in the United Kingdom. Each ADS will also represent any other securities, cash or other property that may be held by the depositary in respect of the ordinary shares deposited with it. The deposited shares together with any other securities, cash or other property held by the depositary are referred to as the deposited securities. The depositary’s office at which the ADSs will be administered and its principal executive office are located at 240 Greenwich Street, New York, NY 10286.
Investors may hold ADSs either: (A) directly (i) by having an American Depositary Receipt, also referred to as an ADR, which is a certificate evidencing a specific number of ADSs, registered in the investors name; or (ii) by having uncertificated ADSs registered in the investors name; or (B) indirectly by holding a security entitlement in ADSs through a broker or other financial institution that is a direct or indirect participant in The Depository Trust Company, also called DTC. If investors hold ADSs directly, it will be the registered ADS holder, also referred to as an ADS holder. This description assumes the investor is an ADS holder. If the investors holds the ADSs indirectly, the investor must rely on the procedures of its broker or other financial institution to assert the rights of ADS holders described in this section. Investors should consult with their broker or financial institution to find out what those procedures are.
Registered holders of uncertificated ADSs will receive statements from the depositary confirming their holdings.
We will not treat the ADS holder as one of our shareholders, and the ADS holder will not have shareholder rights. Scottish law governs the shareholder rights of our company. The depositary will be the holder of the shares underlying the ADSs. As a registered holder of ADSs, the investor only will have ADS holder rights. A deposit agreement among the company, the depositary, ADS holders and all other persons indirectly or beneficially holding ADSs sets out ADS holder rights as well as the rights and obligations of the depositary. New York law governs the deposit agreement and the ADSs.
The following is a summary of the material provisions of the deposit agreement. For more complete information, investors should read the entire deposit agreement and the form of ADR. Portions of this summary description describe matters that may be relevant to the ownership of ADSs but that may not be contained in the deposit agreement.
| 132 |
Dividends and other distributions
The depositary has agreed to pay or distribute to ADS holders the cash dividends or other distributions it or the custodian receives on shares or other deposited securities, upon payment or deduction of its fees, taxes and expenses. investors will receive these distributions in proportion to the number of shares that the ADSs represent.
Cash. The depositary will convert any cash dividend or other cash distribution we pay on the shares into U.S. dollars, if it can do so on a reasonable basis and can transfer the U.S. dollars to the United States. If that is not possible or if any government approval is needed and cannot be obtained, the deposit agreement allows the depositary to distribute the foreign currency only to those ADS holders to whom it is possible to do so. It will hold the foreign currency it cannot convert for the account of the ADS holders who have not been paid. It will not invest the foreign currency and it will not be liable for any interest.
Before making a distribution, any withholding taxes, or other governmental charges that must be paid will be deducted. The depositary will distribute only whole U.S. dollars and cents and will round fractional cents to the nearest whole cent. If the exchange rates fluctuate during a time when the depositary cannot convert the foreign currency, investors lose some of the value of the distribution.
Shares. The depositary may distribute additional ADSs representing any shares we distribute as a dividend or free distribution. The depositary will only distribute whole ADSs. It will sell shares which would require it to deliver a fraction of an ADS (or ADSs representing those shares) and distribute the net proceeds in the same way as it does with cash. If the depositary does not distribute additional ADSs, the outstanding ADSs will also represent the new shares. The depositary may sell a portion of the distributed shares (or ADSs representing those shares) sufficient to pay its fees and expenses in connection with that distribution.
Rights to purchase additional shares. If we offer holders of our securities any rights to subscribe for additional shares or any other rights, the depositary may: (i) exercise those rights on behalf of ADS holders; (ii) distribute those rights to ADS holders; or (iii) sell those rights and distribute the net proceeds to ADS holders, in each case after deduction or upon payment of its fees and expenses. To the extent the depositary does not do any of those things, it will allow the rights to lapse. In that case, investors will receive no value for them. The depositary will exercise or distribute rights only if we ask it to and provide satisfactory assurances to the depositary that it is legal to do so. If the depositary will exercise rights, it will purchase the securities to which the rights relate and distribute those securities or, in the case of shares, new ADSs representing the new shares, to subscribing ADS holders, but only if ADS holders have paid the exercise price to the depositary. U.S. securities laws may restrict the ability of the depositary to distribute rights or ADSs or other securities issued on exercise of rights to all or certain ADS holders, and the securities distributed may be subject to restrictions on transfer.
Other Distributions. The depositary will send to ADS holders anything else we distribute on deposited securities by any means it thinks is legal, fair and practical. If it cannot make the distribution in that way, the depositary has a choice. It may decide to sell what we distributed and distribute the net proceeds, in the same way as it does with cash. Or, it may decide to hold what we distributed, in which case ADSs will also represent the newly distributed property. However, the depositary is not required to distribute any securities (other than ADSs) to ADS holders unless it receives satisfactory evidence from us that it is legal to make that distribution. The depositary may sell a portion of the distributed securities or property sufficient to pay its fees and expenses in connection with that distribution. U.S. securities laws may restrict the ability of the depositary to distribute securities to all or certain ADS holders, and the securities distributed may be subject to restrictions on transfer. The depositary is not responsible if it decides that it is unlawful or impractical to make a distribution available to any ADS holders. We have no obligation to register ADSs, shares, rights or other securities under the Securities Act. We also have no obligation to take any other action to permit the distribution of ADSs, shares, rights or anything else to ADS holders. This means that investors may not receive the distributions we make on our shares or any value for them if it is illegal or impractical for us to make them available to the ADS holder.
| 133 |
Deposit, withdrawal and cancellation
How are the ADSs issued?
The depositary will deliver ADSs if the investor or its broker deposits shares or evidence of rights to receive shares with the custodian. Upon payment of its fees and expenses and of any taxes or charges, such as stamp taxes or stock transfer taxes or fees, the depositary will register the appropriate number of ADSs in the names requested and will deliver the ADSs to or upon the order of the person or persons that made the deposit.
How can ADS holders withdraw the deposited securities?
ADS holders may surrender their ADSs for the purpose of withdrawal at the depositary’s office. Upon payment of its fees and expenses and of any taxes or charges, such as stamp taxes or stock transfer taxes or fees, the depositary will deliver the shares and any other deposited securities underlying the ADSs to the ADS holder or a person the ADS holder designates at the office of the custodian. Or, at the ADS holders request, risk and expense, the depositary will deliver the deposited securities at its office, if feasible. However, the depositary is not required to accept surrender of ADSs to the extent it would require delivery of a fraction of a deposited share or other security. The depositary may charge a fee and its expenses for instructing the custodian regarding delivery of deposited securities.
How do ADS holders interchange between certificated ADSs and uncertificated ADSs?
ADS holders may surrender their ADR to the depositary for the purpose of exchanging the ADR for uncertificated ADSs. The depositary will cancel that ADR and will send to the ADS holder a statement confirming that the ADS holder is the registered holder of uncertificated ADSs. Upon receipt by the depositary of a proper instruction from a registered holder of uncertificated ADSs requesting the exchange of uncertificated ADSs for certificated ADSs, the depositary will execute and deliver to the ADS holder an ADR evidencing those ADSs.
Voting rights
ADS holders may instruct the depositary how to vote the number of deposited shares their ADSs represent. The voting rights of holders of ordinary shares are described in “Description of share capital and articles of association—Articles of association.”
If we request the depositary to solicit voting instructions (and we are not required to do so) from the ADS holders, the depositary will notify them of an annual general meeting and send or make voting materials available to the ADS holders. Those materials will describe the matters to be voted on and explain how the ADS holders may instruct the depositary how to vote. For instructions to be valid, they must reach the depositary by a date set by the depositary. The depositary will try, as far as practical, subject to the laws of Scotland and the provisions of our Articles or similar documents, to vote or to have its agents vote the shares or other deposited securities as instructed by ADS holders. If we do not request the depositary to solicit voting instructions, ADS holder can still send voting instructions, and, in that case, the depositary may try to vote as instructed, but it is not required to do so.
Except by instructing the depositary as described above, ADS holders will not be able to exercise voting rights unless they surrender the ADSs and withdraw the shares. However, the ADS holder may not know about the annual general meeting enough in advance to withdraw the shares. In any event, the depositary will not exercise any discretion in voting deposited securities and it will only vote or attempt to vote as instructed or as described in the following sentence. If we asked the depositary to solicit instructions at least 45 days before the meeting date, but the depositary does not receive voting instructions from the ADS holder by the specified date, it will consider that they have been authorized and directed to give a discretionary proxy to a person designated by us to attend the meeting solely for quorum purposes, but not to vote the ordinary shares on any matter presented to the shareholders.
We cannot give assurance that ADS holders will receive the voting materials in time to ensure that they can instruct the depositary to vote their shares. In addition, the depositary and its agents are not responsible for failing to carry out voting instructions or for the manner of carrying out voting instructions. This means that ADS holders may not be able to exercise voting rights, and there may be nothing an ADS holder can do if the shares are not voted as requested.
In order to give ADS holders a reasonable opportunity to instruct the depositary as to the exercise of voting rights relating to deposited securities, if we request the depositary to act, we agree to give the depositary notice of any such meeting and details concerning the matters to be voted upon at least 45 days in advance of the meeting date.
| 134 |
Fees and expenses
| Persons
depositing or withdrawing shares or ADS holders must pay: |
For: | |
| $5.00 (or less) per 100 ADSs (or portion of 100 ADSs) | Issuance of ADSs, including issuances resulting from a distribution of shares or rights or other property Cancellation of ADSs for the purpose of withdrawal, including if the deposit agreement terminates | |
| $0.05 (or less) per ADS | Any cash distribution to ADS holders | |
| A fee equivalent to the fee that would be payable if securities distributed to the holder had been shares and the shares had been deposited for issuance of ADSs | Distribution of securities distributed to holders of deposited securities (including rights) that are distributed by the depositary to ADS holders | |
| $0.05 (or less) per ADS per calendar year | Depositary services | |
| Registration or transfer fees | Transfer and registration of shares on our share register to or from the name of the depositary or its agent when deposited or withdrawn shares | |
| Expenses of the depositary | Cable (including SWIFT), telex and facsimile transmissions (when expressly provided in the deposit agreement) Converting foreign currency to U.S. dollars | |
| Taxes and other governmental charges the depositary or the custodian has to pay on any ADSs or shares underlying ADSs, such as stock transfer taxes, stamp duty or withholding taxes | As necessary | |
| Any charges incurred by the depositary or its agents for servicing the deposited securities | As necessary | |
The depositary collects its fees for delivery and surrender of ADSs directly from investors depositing shares or surrendering ADSs for the purpose of withdrawal or from intermediaries acting for them. The depositary collects fees for making distributions to investors by deducting those fees from the amounts distributed or by selling a portion of distributable property to pay the fees. The depositary may collect its annual fee for depositary services by deduction from cash distributions or by directly billing investors or by charging the book-entry system accounts of participants acting for them. The depositary may collect any of its fees by deduction from any cash distribution payable (or by selling a portion of securities or other property distributable) to ADS holders that are obligated to pay those fees. The depositary may generally refuse to provide fee-attracting services until its fees for those services are paid.
From time to time, the depositary may make payments to us to reimburse us for costs and expenses generally arising out of establishment and maintenance of the ADS program, waive fees and expenses for services provided to us by the depositary or share revenue from the fees collected from ADS holders. In performing its duties under the deposit agreement, the depositary may use brokers, dealers, foreign currency dealers or other service providers that are owned by or affiliated with the depositary and that may earn or share fees, spreads or commissions.
The depositary may convert currency itself or through any of its affiliates and, in those cases, acts as principal for its own account and not as agent, advisor, broker or fiduciary on behalf of any other person and earns revenue, including, without limitation, transaction spreads, that it will retain for its own account. The revenue is based on, among other things, the difference between the exchange rate assigned to the currency conversion made under the deposit agreement and the rate that the depositary or its affiliate receives when buying or selling foreign currency for its own account. The depositary makes no representation that the exchange rate used or obtained in any currency conversion under the deposit agreement will be the most favorable rate that could be obtained at the time or that the method by which that rate will be determined will be the most favorable to ADS holders, subject to the depositary’s obligations under the deposit agreement. The methodology used to determine exchange rates used in currency conversions is available upon request.
| 135 |
Payment of taxes
ADS holders will be responsible for any taxes or other governmental charges payable on the ADSs or on the deposited securities represented by any of the ADSs. The depositary may refuse to register any transfer of the ADSs or allow a holder to withdraw the deposited securities represented by the ADSs until those taxes or other charges are paid. It may apply payments owed to the holder or sell deposited securities represented by the ADSs to pay any taxes owed and the ADS holder will remain liable for any deficiency. If the depositary sells deposited securities, it will, if appropriate, reduce the number of ADSs to reflect the sale and pay to ADS holders any proceeds, or send to ADS holders any property, remaining after it has paid the taxes.
Tender and exchange offers; redemption, replacement or cancellation of deposited securities
The depositary will not tender deposited securities in any voluntary tender or exchange offer unless instructed to do so by an ADS holder surrendering ADSs and subject to any conditions or procedures the depositary may establish.
If deposited securities are redeemed for cash in a transaction that is mandatory for the depositary as a holder of deposited securities, the depositary will call for surrender of a corresponding number of ADSs and distribute the net redemption money to the holders of called ADSs upon surrender of those ADSs.
If there is any change in the deposited securities such as a sub-division, combination or other reclassification, or any merger, consolidation, recapitalization or reorganization affecting the issuer of deposited securities in which the depositary receives new securities in exchange for or in lieu of the old deposited securities, the depositary will hold those replacement securities as deposited securities under the deposit agreement. However, if the depositary decides it would not be lawful and practical to hold the replacement securities because those securities could not be distributed to ADS holders or for any other reason, the depositary may instead sell the replacement securities and distribute the net proceeds upon surrender of the ADSs.
If there is a replacement of the deposited securities and the depositary will continue to hold the replacement securities, the depositary may distribute new ADSs representing the new deposited securities or ask the ADS holder to surrender their outstanding ADRs in exchange for new ADRs identifying the new deposited securities.
If there are no deposited securities underlying ADSs, including if the deposited securities are cancelled, or if the deposited securities underlying ADSs have become apparently worthless, the depositary may call for surrender of those ADSs or cancel those ADSs upon notice to the ADS holders.
Amendment and termination
How may the deposit agreement be amended?
We may agree with the depositary to amend the deposit agreement and the ADRs without the consent of the ADS holders for any reason. If an amendment adds or increases fees or charges, except for taxes and other governmental charges or expenses of the depositary for registration fees, facsimile costs, delivery charges or similar items, or prejudices a substantial right of ADS holders, it will not become effective for outstanding ADSs until 30 days after the depositary notifies ADS holders of the amendment. At the time an amendment becomes effective, the ADS holder will be considered, by continuing to hold ADSs, to have agreed to the amendment and to be bound by the ADRs and the deposit agreement as amended.
| 136 |
How may the deposit agreement be terminated?
The depositary will initiate termination of the deposit agreement if we instruct it to do so. The depositary may initiate termination of the deposit agreement if:
| ● | 60 days have passed since the depositary told us it wants to resign but a successor depositary has not been appointed and accepted its appointment; | |
| ● | we delist the ADSs from an exchange in the United States on which they were listed and do not list the ADSs on another exchange in the United States or make arrangements for trading of ADSs on the U.S. over-the-counter market; | |
| ● | we delist our shares from an exchange outside the United States on which they were listed and do not list the shares on another exchange outside the United States; | |
| ● | the depositary has reason to believe the ADSs have become, or will become, ineligible for registration on Form F-6 under the Securities Act of 1933, as amended; | |
| ● | we appear to be insolvent or enter insolvency proceedings; | |
| ● | all or substantially all the value of the deposited securities has been distributed either in cash or in the form of securities; | |
| ● | there are no deposited securities underlying the ADSs or the underlying deposited securities have become apparently worthless; or | |
| ● | there has been a replacement of deposited securities. |
If the deposit agreement will terminate, the depositary will notify ADS holders at least 90 days before the termination date. At any time after the termination date, the depositary may sell the deposited securities. After that, the depositary will hold the money it received on the sale, as well as any other cash it is holding under the deposit agreement, unsegregated and without liability for interest, for the pro rata benefit of the ADS holders that have not surrendered their ADSs. Normally, the depositary will sell as soon as practicable after the termination date.
After the termination date and before the depositary sells, ADS holders can still surrender their ADSs and receive delivery of deposited securities, except that the depositary may refuse to accept a surrender for the purpose of withdrawing deposited securities or reverse previously accepted surrenders of that kind that have not settled if it would interfere with the selling process. The depositary may refuse to accept a surrender for the purpose of withdrawing sale proceeds until all the deposited securities have been sold. The depositary will continue to collect distributions on deposited securities, but, after the termination date, the depositary is not required to register any transfer of ADSs or distribute any dividends or other distributions on deposited securities to the ADSs holder (until they surrender their ADSs) or give any notices or perform any other duties under the deposit agreement except as described in this paragraph.
Limitations on obligations and liability
The deposit agreement expressly limits our obligations and the obligations of the depositary. It also limits our liability and the liability of the depositary. We and the depositary:
| ● | are only obligated to take the actions specifically set forth in the deposit agreement without negligence or bad faith, and the depositary will not be a fiduciary or have any fiduciary duty to holders of ADSs; | |
| ● | are not liable if we are or it is prevented or delayed by law or by events or circumstances beyond our or its ability to prevent or counteract with reasonable care or effort from performing our or its obligations under the deposit agreement; | |
| ● | are not liable if we or it exercises discretion permitted under the deposit agreement; |
| 137 |
| ● | are not liable for any action or inaction in reliance on the advice or information received from legal counsel, accountants, any person presenting ordinary shares for deposit, any holder of ADSs or authorized representatives thereof, or any other person believed by either of us in good faith to be competent to give such advice or information; | |
| ● | are not liable for the inability of any holder of ADSs to benefit from any distribution on deposited securities that is not made available to holders of ADSs under the terms of the deposit agreement, or for any special, consequential or punitive damages for any breach of the terms of the deposit agreement; | |
| ● | have no obligation to become involved in a lawsuit or other proceeding related to the ADSs or the deposit agreement on behalf of the ADS holder or on behalf of any other person; | |
| ● | may rely upon any documents we believe or it believes in good faith to be genuine and to have been signed or presented by the proper person; | |
| ● | are not liable for the acts or omissions of any securities depository, clearing agency or settlement system; and | |
| ● | the depositary has no duty to make any determination or provide any information as to our tax status, or any liability for any tax consequences that may be incurred by ADS holders as a result of owning or holding ADSs or be liable for the inability or failure of an ADS holder to obtain the benefit of a foreign tax credit, reduced rate of withholding or refund of amounts withheld in respect of tax or any other tax benefit. |
In the deposit agreement, we and the depositary agree to indemnify each other under certain circumstances.
Requirements for depositary actions
Before the depositary will deliver or register a transfer of ADSs, make a distribution on ADSs, or permit withdrawal of shares, the depositary may require:
| ● | payment of stock transfer or other taxes or other governmental charges and transfer or registration fees charged by third parties for the transfer of any shares or other deposited securities; | |
| ● | satisfactory proof of the identity and genuineness of any signature or other information it deems necessary; and | |
| ● | compliance with regulations it may establish, from time to time, consistent with the deposit agreement, including presentation of transfer documents. |
The depositary may refuse to deliver ADSs or register transfers of ADSs when the transfer books of the depositary or our transfer books are closed or at any time if the depositary or we think it advisable to do so.
Right to receive the shares underlying ADSs
ADS holders have the right to cancel their ADSs and withdraw the underlying shares at any time except:
| ● | when temporary delays arise because: (i) the depositary has closed its transfer books or we have closed our transfer books; (ii) the transfer of shares is blocked to permit voting at an annual general meeting; or (iii) we are paying a dividend on our shares; | |
| ● | when the ADS holder owes money to pay fees, taxes and similar charges; or | |
| ● | when it is necessary to prohibit withdrawals in order to comply with any laws or governmental regulations that apply to ADSs or to the withdrawal of shares or other deposited securities. |
This right of withdrawal may not be limited by any other provision of the deposit agreement.
| 138 |
Direct registration system
In the deposit agreement, all parties to the deposit agreement acknowledge that the Direct Registration System, also referred to as DRS, and Profile Modification System, also referred to as Profile, will apply to the ADSs. DRS is a system administered by DTC that facilitates interchange between registered holding of uncertificated ADSs and holding of security entitlements in ADSs through DTC and a DTC participant. Profile is a feature of DRS that allows a DTC participant, claiming to act on behalf of a registered holder of uncertificated ADSs, to direct the depositary to register a transfer of those ADSs to DTC or its nominee and to deliver those ADSs to the DTC account of that DTC participant without receipt by the depositary of prior authorization from the ADS holder to register that transfer.
In connection with and in accordance with the arrangements and procedures relating to DRS/Profile, the parties to the deposit agreement understand that the depositary will not determine whether the DTC participant that is claiming to be acting on behalf of an ADS holder in requesting registration of transfer and delivery as described in the paragraph above has the actual authority to act on behalf of the ADS holder (notwithstanding any requirements under the Uniform Commercial Code). In the deposit agreement, the parties agree that the depositary’s reliance on and compliance with instructions received by the depositary through the DRS/Profile system and in accordance with the deposit agreement will not constitute negligence or bad faith on the part of the depositary.
Books of depositary; shareholder communications; inspection of register of holders of ADSs
The depositary will maintain ADS holder records at its depositary office. The depositary will make available for inspection at its office all communications that it receives from us as a holder of deposited securities that we make generally available to holders of deposited securities. The depositary will send copies of those communications or otherwise make those communications available to ADS holders if we ask it to. ADS holders have a right to inspect the register of holders of ADSs, but not for the purpose of contacting those holders about a matter unrelated to our business or the ADSs.
Jury trial waiver
The deposit agreement provides that, to the extent permitted by law, ADS holders waive the right to a jury trial of any claim they may have against us or the depositary arising out of or relating to our shares, the ADSs or the deposit agreement, including any claim under the U.S. federal securities laws. If we or the depositary opposed a jury trial demand based on the waiver, the court would determine whether the waiver was enforceable in the facts and circumstances of that case in accordance with applicable case law.
ADS holders will not, by agreeing to the terms of the deposit agreement, be deemed to have waived our or the depositary’s compliance with U.S. federal securities laws or the rules and regulations promulgated thereunder.
Public Warrants
The following is a brief summary of certain terms and conditions of the public Warrants and is subject in all respects to the provisions contained in the public Warrant Agent Agreement. Investors should review a copy of the form of Warrant and Warrant Agent Agreement filed with the SEC for a complete description of the terms and conditions applicable to the Warrants.
Form. The Warrants will be issued in electronic certificated form. Warrant holders, however, may request a certificated form of Warrant.
Term. The Warrants will be exercisable on the date of issuance and will expire on the sixth anniversary of the date of issuance.
| 139 |
Exercisability. The Warrants will be exercisable, at the option of each holder, by delivering to us a duly executed exercise notice and cash payment in full for the number of ADSs purchased upon such exercise. We are required to maintain a registration statement to be effective at the time a Warrant may be exercised, and if we do not do so, then the Warrants will have a net-exercise right. The net-exercise basis is based on a formula using the VWAP immediately prior to exercise. The original Holder has paid $0.005 towards the nominal value of the Warrant Shares to be used in the event of a cashless exercise and, no additional consideration for the nominal value shall be required to be paid by the Holder to effect an exercise of this Warrant. The Holder shall not be entitled to the return or refund of all, or any portion, of such pre-funded nominal value under any circumstance or for any reason whatsoever, including in the event this Warrant shall not have been exercised prior to the Termination Date. If the Warrants are not exercised before they expire, in six years, the Warrants will expire and be of no further value and all the rights under the Warrants will terminate. We do not intend to offer any “broker protect period” or other exceptions for not timely exercising a Warrant after they expire; therefore investors should monitor, with their broker, the expiration date and take steps to exercise the Warrant on a timely basis.
Exercise Price. The exercise price of the Warrants is $4.25 per ADS. The exercise price is subject to appropriate adjustment in the event of certain stock splits, stock combinations, stock dividends, recapitalizations or otherwise. The exercise price will also be downward adjusted if we, or through a subsidiary, sell or enter into an agreement to sell, grant an option to sell, reprice an outstanding security to acquire ordinary shares at a price less than $4.25. The downward adjustment will to the price of the newly issued security or adjusted price of the outstanding security, but not less than a floor price set forth in the terms of the Warrants, which is subject to adjustment for stock splits, combinations and recapitalizations, as above. The downward adjustment will not be made if the Company entered into certain delineated types of transactions, including employment related option and similar security grants, exercise of such options and security grants, exercises of currently outstanding securities so long as not repriced, and issuances for acquisitions, strategic transactions, vendors, equipment leasing, licensing, collaborations, and the like so long as they are non-capital raising transactions.
Delivery of ADSs. We shall cause our Depositary to deliver the ADSs for the ordinary shares underlying the Warrants to the holders exercising Warrants by no later than 5:00 P.M. New York City time on the fifth trading day following the Warrants exercise date, provided the funds in payment of the exercise price for such Warrants have cleared on the trading day following the exercise date.
No Fractional Shares. No fractional shares or scrip representing fractional shares shall be issued upon the exercise of the Warrants, and the number of Warrants will be rounded to the nearest whole number.
Transferability. Subject to applicable laws and the restriction on transfer set forth in the Warrant, the Warrant may be transferred at the option of the holder in accordance with the procedures set forth in the Warrant.
Authorized Shares. During the period the Warrants are outstanding, we will reserve from our authorized and unissued ordinary shares a sufficient number of shares to provide for the issuance of the ADSs underlying the Warrants upon the exercise of the Warrants.
Subsequent Rights Offerings. Warrant holders will be entitled to be distributed any purchase rights that the Company distributes generally to its holders of ordinary shares or other securities, which rights will be on the same terms.
Pro Rata Distributions. Warrant holders will be entitled to distributions by the Company, in the manner of dividends and other forms of property or assets distributed to the holders of ordinary shares in proportion to the ADS acquirable upon complete exercise of the Warrants.
Fundamental Transactions. In the event of any corporate transaction, as described in the Warrant Agent Agreement and generally including, a reclassification of our capital, any merger, combination or consolidation with or into another entity, sale of all or substantially all of our assets, tender offer or exchange offer, then the holder shall have the right to receive for each ordinary share that would have been issuable upon exercise of the Warrants immediately prior to the occurrence of the corporate transaction, the number of ordinary shares of the successor or acquiring corporation and any additional consideration receivable upon or as a result of such transaction by a holder of the number of ordinary shares for which the Warrant is exercisable immediately prior to such event. At the Warrant holder’s option, exercisable at any time concurrently with, or within 30 days after, the consummation of a fundamental transaction, the company or successor entity shall purchase the Warrant from the holder by paying an amount of cash equal to the Black Scholes Value (as defined in and calculated under the terms of the Warrant) of the remaining unexercised portion of the Warrant on the date of the consummation of the fundamental transaction; provided, if the fundamental transaction is not within the company’s control, including not approved by the company’s board of directors, the holder shall only be entitled to receive from the Company or any successor entity the same type or form of consideration (and in the same proportion), at the Black Scholes Value of the unexercised portion of the Warrant, that is being offered and paid to the holders of ordinary shares of the Company in connection with the fundamental transaction, whether that consideration be in the form of cash, stock or any combination thereof, or whether the holders of ordinary shares are given the choice to receive from among alternative forms of consideration in connection with the fundamental transaction; provided, further, that if holders of ordinary shares are not offered or paid any consideration in such fundamental transaction, the holders will be deemed to have received common stock of the successor entity.
| 140 |
Right as a Shareholder. Except as otherwise provided in the Warrants or by virtue of such holder’s ownership of our ordinary shares, the holders of the Warrants do not have the rights or privileges of holders of our ADSs until they receive the ADSs underlying the Warrants.
Waivers and Amendments. Any term of the Warrants may be amended or waived with the written consent of holders of the Warrants.
Warrant Agent. The warrant agent for the Warrants is Computershare Inc., a Delaware corporation, and its wholly owned subsidiary, Computershare Trust Company, N.A., a federally chartered trust company
| C. | Material Contracts |
Except as otherwise disclosed in this Annual Report (including the exhibits thereto) and as otherwise described in and filed with our other SEC filings, we are not currently, and have not been in the last two years, party to any material contract, other than contracts entered into in the ordinary course of our business.
| D. | Exchange Controls |
There are no governmental laws, decrees, regulations or other legislation in the United Kingdom that may affect the import or export of capital, including the availability of cash and cash equivalents for use by us, or that may affect the remittance of dividends, interest, or other payments by us to non-resident holders of our ordinary shares or ADSs, other than withholding tax requirements. There is no limitation imposed by English law or our articles of association on the right of non-residents to hold or vote shares.
| E. | Taxation |
U.S. Federal Income Taxes
The following is a summary of the material U.S. federal income tax consequences to U.S. Holders (as defined below) of purchasing, owing and disposing of the ordinary shares, ADSs or Warrants. This discussion is included for general informational purposes only, does not purport to consider all aspects of U.S. federal income taxation that might be relevant to a U.S. Holder, and does not constitute, and is not, a tax opinion for or tax advice to any particular U.S. Holder of ordinary shares, the ADSs or Warrants. The summary does not address any U.S. tax matters other than those specifically discussed. The summary is based on the provisions of the U.S. Internal Revenue Code of 1986, as amended (the “Code”), existing, temporary and proposed Treasury Regulations issued thereunder, judicial decisions and administrative rulings and pronouncements and other legal authorities, all as of the date hereof and all of which are subject to change, possibly with retroactive effect. Any such change could alter the tax consequences described herein.
The discussion below applies only to U.S Holders as capital assets within the meaning of Section 1221 of the Code (generally, property held for investment), and does not address the tax consequences that may be relevant to U.S. Holders who, in light of their particular circumstances, may be subject to special tax rules, including without limitation:
| ● | insurance companies, tax-exempt organizations, regulated investment companies, real estate investment trusts, brokers or dealers in securities or foreign currencies, banks and other financial institutions, mutual funds, retirement plans, traders in securities that elect to mark to market, certain former U.S. citizens or long-term residents; |
| 141 |
| ● | U.S. Holders that are classified for U.S. federal income tax purposes as partnerships and other pass-through entities and investors therein; | |
| ● | U.S. Holders who hold ordinary shares, ADSs or Warrants as part of a hedge, straddle, constructive sale, conversion, or other integrated or risk-reduction transaction, as “qualified small business stock,” within the meaning of Section 1202 of the Code or as Section 1244 stock for purposes of the Code; | |
| ● | U.S. Holders who hold ordinary shares, ADSs or Warrants through individual retirement or other tax-deferred accounts; | |
| ● | U.S. Holders that have a functional currency other than the U.S. dollar; | |
| ● | U.S. Holders who are subject to the alternative minimum tax provisions of the Code or the tax on net investment income imposed by Section 1411 of the Code; | |
| ● | U.S. Holders who acquire their ordinary shares, ADSs or Warrants pursuant to any employee share option or otherwise as compensation; | |
| ● | U.S. Holders required to accelerate the recognition of any item of gross income with respect to their ordinary shares, ADSs or Warrants as a result of such income being recognized on an applicable financial statement; or | |
| ● | U.S. Holders who hold or held, directly or indirectly, or are treated as holding or having held under applicable constructive attribution rules, 10% or more of the ordinary shares, ADSs Warrants of the company, measured by voting power or value. |
Any such U.S. Holders should consult their own tax advisors.
For purposes of this discussion, a “U.S. Holder” means a holder of our ordinary shares, ADSs or Warrants that is or is treated as, for U.S. federal income tax purposes, (i) an individual citizen or resident of the United States, (ii) a corporation (or other entity taxable as a corporation for U.S. federal income tax purposes) created or organized in or under the laws of the United States, any State thereof or the District of Columbia or any entity treated as such for U.S. federal income tax purposes, (iii) an estate the income of which is subject to U.S. federal income taxation regardless of its source, or (iv) a trust (A) the administration over which a U.S. court exercises primary supervision and all of the substantial decisions of which one or more U.S. persons have the authority to control, or (B) that has a valid election in effect under the applicable Treasury Regulations to be treated as a U.S. person under the Code.
If a partnership or other pass-through entity (including any entity or arrangement treated as such for purposes of U.S. federal income tax law) holds our ordinary shares, ADSs or Warrants, the tax treatment of a partner of such partnership or member of such entity will generally depend upon the status of the partner and the activities of the partnership. Partnerships and other pass-through entities holding our ordinary shares, ADSs or Warrants, and any person who is a partner or member of such entities should consult their own tax advisors regarding the tax consequences of purchasing, owning and disposing of the ordinary shares, ADSs or Warrants.
Passive Foreign Investment Company Considerations
A non-U.S. corporation, such as TCB, will be classified as a passive foreign investment company, or PFIC, for U.S. federal income tax purposes, if, in the case of any particular taxable year, either (i) 75% or more of its gross income for such taxable year consists of certain types of “passive” income or (ii) 50% or more of the value of its assets (based on an average of the quarterly values of the assets) during such taxable year is attributable to assets that produce or are held for the production of passive income. For this purpose, cash is categorized as a passive asset and the company’s un-booked intangibles associated with active business activities may generally be classified as active assets. Passive income generally includes, among other things, dividends, interest, rents, royalties, and gains from the disposition of passive assets. For this purpose, a foreign corporation will be treated as owning its proportionate share of the assets and earning its proportionate share of the income of any other non-U.S. corporation in which it owns, directly or indirectly, more than 25% (by value) of the stock.
| 142 |
Based upon its current income and assets and projections as to the value of the ordinary shares or ADSs, it is not presently expected that we will be classified as a PFIC for the 2021 taxable year or the foreseeable future.
The determination of whether we will be or become a PFIC will depend upon the composition of its income (which may differ from our historical results and current projections) and assets and the value of its assets from time to time, including, in particular the value of its goodwill and other un-booked intangibles (which may depend upon the market value of the ordinary shares or ADSs from time to time and may be volatile). Among other matters, if our market capitalization is less than anticipated or subsequently declines, we may be classified as a PFIC for the taxable year in the 2021 taxable year or future taxable years. It is also possible that the IRS may challenge the classification or valuation of our assets, including its goodwill and other unbooked intangibles, or the classification of certain amounts received by us, including interest earnings, which may result in our being, or becoming classified as, a PFIC for the taxable year in 2021 or future taxable years.
The determination of whether we will be or become a PFIC may also depend, in part, on how, and how quickly, it uses liquid assets and the cash proceeds of the IPO or otherwise. If we were to retain significant amounts of liquid assets, including cash, the risk of our being classified as a PFIC may substantially increase. Because there are uncertainties in the application of the relevant rules and PFIC status is a factual determination made annually after the close of each taxable year, there can be no assurance that we will not be a PFIC for the 2021 taxable year or any future taxable year, and no opinion of counsel has or will be provided regarding the classification of us as a PFIC. If we were classified as a PFIC for any year during which a holder held our ordinary shares or ADSs, it generally would continue to be treated as a PFIC for all succeeding years during which such holder held the ordinary shares or ADSs. The discussion below under “—Dividends Paid on Ordinary Shares or ADSs” and “—Sale or Other Disposition of Ordinary Shares or ADS” is written on the basis that we will not be classified as a PFIC for U.S. federal income tax purposes.
Dividends Paid on Ordinary Shares or ADSs
Subject to the PFIC rules described below, any cash distributions (including constructive distributions) paid on the ordinary shares or ADSs out of our current or accumulated earnings and profits, as determined under U.S. federal income tax principles, will generally be includible in the gross income of a U.S. Holder as dividend income on the day actually or constructively received by the U.S. Holder, in the case of ordinary shares or ADSs. Because we does not intend to determine its earnings and profits on the basis of U.S. federal income tax principles, any distribution will generally be treated as a “dividend” for U.S. federal income tax purposes. Under current law, a non-corporate recipient of a dividend from a “qualified foreign corporation” will generally be subject to tax on the dividend income at the lower applicable net capital gains rate rather than the marginal tax rates generally applicable to ordinary income provided that certain holding period and other requirements are met.
A non-U.S. corporation (other than a corporation that is classified as a PFIC for the taxable year in which the dividend is paid or the preceding taxable year) will generally be considered to be a qualified foreign corporation (i) if it is eligible for the benefits of a comprehensive tax treaty with the United States which the Secretary of Treasury of the United States determines is satisfactory for purposes of this provision and which includes an exchange of information program, or (ii) with respect to any dividend it pays on stock, which is readily tradable on an established securities market in the United States. We believe we are eligible for the benefits of the Convention Between the Government of the United States of America and the Government of the United Kingdom of Great Britain and Northern Ireland for the Avoidance of Double Taxation and the Prevention of Fiscal Evasion with Respect to Taxes on Income and On Capital Gains, or the United States-United Kingdom income tax treaty (which the Secretary of the Treasury of the United States has determined is satisfactory for this purpose and includes an exchange of information program), in which case it would be treated as a qualified foreign corporation with respect to dividends paid on the ordinary shares or ADSs. U.S. Holders are urged to consult their tax advisors regarding the availability of the reduced tax rate on dividends in their particular circumstances. Dividends received on the ordinary shares will not be eligible for the dividends received deduction allowed to corporations.
| 143 |
Sale or Other Disposition of Ordinary Shares, ADSs or Warrants
Subject to the PFIC rules discussed below, a U.S. Holder of our ordinary shares, ADRs or Warrants will generally recognize capital gain or loss, if any, upon the sale or other disposition of ordinary shares, ADSs or Warrants, respectively, in an amount equal to the difference between the amount realized upon the disposition and the U.S. Holder’s adjusted tax basis in such ordinary shares, ADSs or Warrants. Any capital gain or loss will be long-term capital gain or loss if the ordinary shares, ADSs or Warrants have been held for more than one year and will generally be United States source capital gain or loss for United States foreign tax credit purposes. Long-term capital gains of non-corporate taxpayers are currently eligible for reduced rates of taxation.
Exercise and Expiration of Warrants
In general, a U.S. Holder will not recognize gain or loss for U.S. federal income tax purposes upon exercise of a Warrant. The U.S. Holder will take a tax basis in the ADSs acquired on the exercise of a Warrant equal to the exercise price of the Warrant, increased by the U.S. Holder’s adjusted tax basis in the Warrant exercised (as determined pursuant to the rules discussed below on allocation of purchase price). The U.S. Holder’s holding period in the ADSs acquired on exercise of the Warrant will begin on the date of exercise of the Warrant and will not include any period for which the U.S. Holder held the Warrant.
The lapse or expiration of a Warrant will be treated as if the U.S. Holder sold or exchanged the Warrant and recognized a capital loss equal to the U.S. Holder’s tax basis in the Warrant.
Disposition of Foreign Currency
U.S. Holders are urged to consult their tax advisors regarding the tax consequences of receiving, converting or disposing of any non-U.S. currency received as dividends on our ordinary shares or ADSs.
Tax on Net Investment Income
Additional 3.8% Medicare tax on some or all of such U.S. Holder’s “net investment income.” Net investment income generally includes income from the ordinary shares, ADSs or Warrants unless such income is derived in the ordinary course of the conduct of a trade or business (other than a trade or business that consists of certain passive or trading activities). You should consult your tax advisors regarding the effect this Medicare tax may have, if any, on your acquisition, ownership or disposition of ordinary shares, ADSs or Warrants.
Passive Foreign Investment Company Rules
If we are is classified as a PFIC for any taxable year during which a U.S. Holder holds our ordinary shares or ADSs, unless the holder makes a mark-to-market election (as described below), the holder will, except as discussed below, be subject to special tax rules that have a penalizing effect, regardless of whether we remain a PFIC, on (i) any excess distribution that we make to the holder (which generally means any distribution paid during a taxable year to a holder that is greater than 125% of the average annual distributions paid in the three preceding taxable years or, if shorter, the holder’s holding period for the ordinary shares or ADSs), and (ii) any gain realized on the sale or other disposition, including, under certain circumstances, a pledge, of our ordinary shares or ADSs. Under the PFIC rules:
| ● | The excess distribution and/or gain will be allocated ratably over the U.S. Holder’s holding period for the ordinary shares or ADSs; | |
| ● | The amount of the excess distribution or gain allocated to the taxable year of the distribution or disposition and any taxable years in the U.S. Holder’s holding period prior to the first taxable year in which we are classified as a PFIC, or a pre-PFIC year, will be taxable as ordinary income; and | |
| ● | The amount of the excess distribution or gain allocated to each taxable year other than the taxable year of the distribution or disposition or a pre-PFIC year, will be subject to tax at the highest tax rate in effect applicable to the individuals or corporations, and the interest charge generally applicable to underpayments of tax will be imposed on the resulting tax attributable to each such year. |
| 144 |
If we are a PFIC for any taxable year during which a U.S. Holder holds our ordinary shares or ADSs and any of its non-U.S. subsidiaries is also a PFIC, such holder would be treated as owning a proportionate amount (by value) of the shares of the lower-tier PFIC for purposes of the application of these rules. Each U.S. Holder is advised to consult its tax advisors regarding the application of the PFIC rules to any of our subsidiaries.
A U.S. holder of the Warrants is taxed in a manner similar to a U.S. holder of common shares if the holder realizes gain on the sale of the Warrants. If the holder of the warrants exercises the warrants to purchase common shares, the holding period over which any income realized is allocated includes the holding period of the warrants. The U.S. warrant holder is treated as a holder of PFIC stock taxable under the ordinary income allocation and interest charge regime described herein.
As an alternative to the foregoing rules, a U.S. Holder of “marketable stock” in a PFIC may make a mark-to-market election with respect to such ordinary shares or ADSs, provided that they are “regularly traded” (as specially defined under the Code) on The NASDAQ Stock Market. No assurances may be given regarding whether the ordinary shares or ADSs will qualify, or will continue to be qualified, as being regularly traded in this regard. If a mark-to-market election is made, the U.S. Holder will generally (i) include as ordinary income for each taxable year that we are a PFIC the excess, if any, of the fair market value of ordinary shares or ADSs held at the end of the taxable year over the adjusted tax basis of such securities and (ii) deduct as an ordinary loss the excess, if any, of the adjusted tax basis of such securities over the fair market value of such securities held at the end of the taxable year, but only to the extent of the net amount previously included in income as a result of the mark-to-market election. The U.S. Holder’s adjusted tax basis in the ordinary shares or ADSs would be adjusted to reflect any income or loss resulting from the mark-to-market election. If a U.S. Holder makes an effective mark-to-market election, in each year that we are a PFIC any gain recognized upon the sale or other disposition of the ordinary shares or ADSs will be treated as ordinary income and loss will be treated as ordinary loss, but only to the extent of the net amount previously included in income as a result of the mark-to-market election. U.S. Holders of our ordinary shares or ADSs should consult their tax advisors regarding the availability of a mark-to-market election with respect to such ordinary shares or ADSs.
If a U.S. Holder makes a mark-to-market election in respect of a corporation classified as a PFIC and such corporation ceases to be classified as a PFIC, the holder will not be required to take into account the mark-to-market gain or loss described above during any period that such corporation is not classified as a PFIC.
Because a mark-to-market election cannot be made for any lower-tier PFICs that a PFIC may own, a U.S. Holder who makes a mark-to-market election with respect to the ordinary shares or ADSs may continue to be subject to the general PFIC rules with respect to such holder’s indirect interest in any of our non-U.S. subsidiaries that is classified as a PFIC.
We do not intend to provide information necessary for U.S. Holder’s to make qualified electing fund elections, which, if available, would result in tax treatment different from the general tax treatment for PFICs described above. However, as described above under “Passive Foreign Investment Company Considerations-PFIC Classification of TCB,” it is not presently expected that we will be classified as a PFIC for the 2021 taxable year or the foreseeable future.
As discussed above under “Dividends Paid on Ordinary Shares or ADSs”, dividends that we pay on the ordinary shares or ADSs will not be eligible for the reduced tax rate that applies to qualified dividend income if we are is classified as a PFIC for the taxable year in which the dividend is paid or the preceding taxable year. In addition, if a U.S. Holder owns the ordinary shares or ADSs during any taxable year that we are a PFIC, the holder must file an annual information return with the IRS. Each holder is urged to consult its tax advisor concerning the U.S. federal income tax consequences of purchasing, holding, and disposing ordinary shares or ADSs if we are or become a PFIC, including the possibility of making a mark-to-market election and the unavailability of the qualified electing fund election.
| 145 |
Information reporting and backup withholding
Certain U.S. Holders are required to report information to the IRS relating to an interest in “specified foreign financial assets,” including shares issued by a non-U.S. corporation, for any year in which the aggregate value of all specified foreign financial assets exceeds $50 thousand (or a higher U.S. dollar amount prescribed by the IRS), subject to certain exceptions (including an exception for shares held in custodial accounts maintained with a United States financial institution). These rules also impose penalties if a holder is required to submit such information to the IRS and fails to do so.
In addition, U.S. Holders may be subject to information reporting to the IRS and backup withholding with respect to dividends on and proceeds from the sale or other disposition of the our ordinary shares, ADSs or Warrants. Information reporting will apply to payments of dividends on, and to proceeds from the sale or other disposition of, our ordinary shares, ADSs or Warrants by a paying agent within the United States to a holder, other than holders that are exempt from information reporting and properly certify their exemption. A paying agent within the United States will be required to withhold at the applicable statutory rate, currently 24%, in respect of any payments of dividends on, and the proceeds from the disposition of, our ordinary shares, ADRs or Warrants within the U.S. to a U.S. Holder (other than holders that are exempt from backup withholding and properly certify their exemption) if the holder fails to furnish its correct taxpayer identification number or otherwise fails to comply with applicable backup withholding requirements. U.S. Holders who are required to establish their exempt status generally must provide a properly completed IRS Form W-9.
Backup withholding is not an additional tax. Amounts withheld as backup withholding may be credited against a holder’s U.S. federal income tax liability. A U.S. Holder generally may obtain a refund of any amounts withheld under the backup withholding rules by filing the appropriate claim for refund with the IRS in a timely manner and furnishing any required information. Each U.S. Holder is advised to consult with its tax advisor regarding the application of the United States information reporting rules to their particular circumstances.
Material United Kingdom Tax Considerations
The following is a description of the material U.K. tax considerations relating primarily to the ownership and disposal of our ordinary shares, ADSs or Warrants by the U.S. Holders described above. The U.K. tax comments set out below are based on current U.K. tax law as applied in Scotland, and HMRC practice (which may not be binding on HMRC) as at the date of this summary, both of which are subject to change, possibly with retrospective effect. They are intended as a general guide and, save where otherwise stated, only apply to you if you are not resident in the U.K. for U.K. tax purposes and do not hold our ordinary shares, ADSs or Warrants for the purposes of a trade, profession or vocation that you carry on in the U.K. through a branch, agency or permanent establishment in the U.K. and if you hold our ordinary shares as an investment for U.K. tax purposes and are not subject to special rules.
This summary does not address all possible tax consequences relating to an investment in our ordinary shares, ADSs or Warrants. In particular it does not cover the U.K. inheritance tax consequences of holding our ordinary shares, ADSs or Warrants. It assumes that the depositary or DTC has not made an election under section 97A(1) of the Finance Act 1986. It assumes that we do not (and will not at any time) derive 75% or more of our qualifying asset value, directly or indirectly, from U.K. land, and that we are and remain solely resident in the U.K. for tax purposes. It assumes that the holder is not our officer or our employee (or of any related company of ours) and has not (and is not deemed to have) acquired the ordinary shares, ADSs or Warrants by virtue of an office or employment. It assumes that a holder of ordinary shares or ADSs is the beneficial owner of the underlying ordinary shares for U.K. tax purposes. This summary is for general information only and is not intended to be, nor should it be considered to be, legal or tax advice to any particular holder. Holders of our ordinary shares, ADSs or Warrants are strongly urged to consult their tax advisers in connection with the U.K. tax consequences of their investment in our securities.
U.K. Taxation of Dividends and Distributions
We will not be required to withhold amounts for or on account of U.K. tax at source when paying a dividend or distribution in respect of our ordinary shares.
Individual holders who hold our ordinary shares as an investment, who are not resident in the U.K. for U.K. tax purposes should not be subject to U.K. income tax in respect of any dividends on our ordinary shares, unless they hold their ordinary shares in connection with any trade, profession or vocation carried on (whether solely or in partnership) by them in the U.K. through a branch, agency or permanent establishment in the U.K.. In these circumstances, such holder may, depending on his or her individual circumstances, be chargeable to U.K. income tax in respect of our dividends.
| 146 |
Corporate holders which are not resident in the U.K. for U.K. tax purposes should not be subject to U.K. corporation tax in respect of any dividends on our ordinary shares, unless they carry on a trade in the U.K. through a permanent establishment to which the ordinary shares are attributable. In these circumstances, such holders may, depending on their individual circumstances and if an exemption from U.K. corporation tax in respect of dividend payments does not apply, be chargeable to U.K. corporation tax in respect of our dividends.
U.K. Taxation of Capital Gains
An individual holder who is not resident in the U.K. for U.K. tax purposes should not be liable to U.K. capital gains tax on capital gains realized on the disposal of their ordinary shares unless such holder carries on (whether solely or in partnership) a trade, profession or vocation in the U.K. through a branch or agency in the U.K. to which our ordinary shares are attributable. In these circumstances, such holder may, depending on his or her individual circumstances, be chargeable to U.K. capital gains tax on chargeable gains arising from a disposal of his or her ordinary shares.
Any such individual holder of our ordinary shares who is temporarily non-resident for U.K. tax purposes will, in certain circumstances, become liable to U.K. tax on capital gains in respect of gains realized while they were not resident in the U.K.
A corporate holder of our ordinary shares which is not resident in the U.K. for U.K. tax purposes should not be liable for U.K. corporation tax on chargeable gains realized on the disposal of our ordinary shares unless it carries on a trade in the U.K. through a permanent establishment in the U.K. to which our ordinary shares are attributable. In these circumstances, a disposal of ordinary shares by such holder may give rise to a chargeable gain or an allowable loss for the purposes of U.K. corporation tax.
Stamp Duty and Stamp Duty Reserve Tax
The discussion below relates to the holders of our ordinary shares or ADSs wherever resident, however it should be noted that special rules may apply to certain persons such as market makers, brokers, dealers or intermediaries.
As a general rule (and except in relation to depositary receipt systems and clearance services (as to which see below)), no UK stamp duty or stamp duty reserve tax, or SDRT, is payable on the issue of the ordinary shares underlying the ADSs.
An unconditional agreement to transfer ordinary shares will normally give rise to a charge to SDRT at the rate of 0.5% of the amount or value of the consideration payable for the transfer. The purchaser of the shares is liable for the SDRT. Transfers of ordinary shares in certificated form are generally also subject to stamp duty at the rate of 0.5% of the amount or value of the consideration given for the transfer (rounded up to the next £5.00). Stamp duty is normally paid by the purchaser. The charge to SDRT will be cancelled or, if already paid, repaid (generally with interest), where a transfer instrument has been duly stamped within six years of the charge arising, (either by paying the stamp duty or by claiming an appropriate relief) or if the instrument is otherwise exempt from stamp duty.
Under current UK legislation, an issue or transfer of ordinary shares or an unconditional agreement to transfer ordinary shares to a clearance service or a depositary receipt system (including to a nominee or agent for, a person whose business is or includes the issue of depositary receipts or the provision of clearance services) will generally be subject to SDRT (and, in the case of transfers, where the transfer is effected by a written instrument, stamp duty) at a higher rate of 1.5% of the amount or value of the consideration given for the transfer or, in certain circumstances, the value of the ordinary shares unless the clearance service has made and maintained an election under section 97A of the UK Finance Act 1986, or a section 97A election. It is understood that HMRC regards the facilities of DTC as a clearance service for these purposes and we are not aware of any section 97A election having been made by the DTC.
| 147 |
However, based on current published HMRC practice following European Union case law in respect of the European Council Directives 69/335/EEC and 2009/7/EC, no SDRT is generally payable in respect of such an issue of ordinary shares and no SDRT or stamp duty is generally payable in respect of such a transfer of ordinary shares where such transfer is an integral part of an issue of share capital. It is noted that on January 31, 2020 the United Kingdom ceased to be a Member State of the European Union. Accordingly, the extent to which HMRC’s position will remain as set out in this paragraph following the end of the transition period on December 31, 2020 is uncertain.
Any stamp duty or SDRT payable on an issue or transfer of ordinary shares to a depositary receipt system or clearance service (although strictly accountable by the clearance service or depositary receipt system operator or their nominee) will in practice generally be paid by the transferors or participants in the clearance service or depositary receipt system. Specific professional advice should be sought before incurring or reimbursing the costs of a 1.5% stamp duty or SDRT charge in any circumstances.
No UK SDRT or stamp duty is required to be paid in respect of the issue or transfer of, or an agreement to transfer, ADSs (including by way of a paperless transfer of ADSs through the facilities of DTC).
| F. | Dividend and Paying Agents |
Not applicable.
| G. | Statement of Experts |
Not applicable.
| H. | Documents on Display |
We are subject to the informational requirements of the Exchange Act. Accordingly, we are required to file reports and other information with the SEC, including annual reports on Form 20-F and reports on Form 6-K. You may inspect and copy reports and other information filed with the SEC at the Public Reference Room at 100 F Street, N.E., Washington, D.C. 20549. Information on the operation of the Public Reference Room may be obtained by calling the SEC at 1-800-732-0330. In addition, the SEC maintains an Internet website that contains reports and other information about issuers, like us, that file electronically with the SEC. The address of that website is www.sec.gov.
We also make available on our website, free of charge, our Annual Report and the text of our reports on Form 6-K, including any amendments to these reports, as well as certain other SEC filings, as soon as reasonably practicable after they are electronically filed with or furnished to the SEC. Our website address is https://tcbiopharm.com. The information contained on our website is not incorporated by reference in this Annual Report.
| I. | Subsidiary Information |
Not applicable.
| Item 11. | Quantitative and Qualitative Disclosures about Market Risk |
We are exposed to a variety of risks in the ordinary course of our business, including, but not limited to, currency risk, liquidity risk and credit risk, as discussed below. We regularly assess each of these risks to minimize any adverse effects on our business as a result of those factors. See Note 22 to our audited consolidated financial statements for further discussion of our exposure to these risks.
Credit risk
Credit risk is the risk of financial loss to the Company if a customer or counterparty to a financial instrument fails to meet its contractual obligations, and arises principally from the Company’s receivables from customers and from its financing activities, including deposits with banks and financial institutions, foreign exchange transactions and other financial instruments. The Company only engages with banks and financial institutions with a Standard and Poor credit rating of BBB or greater.
| 148 |
The Company has a small number of customers as part of its collaboration agreements. To manage the credit risks around collaboration agreements the Company will assess the creditworthiness of partners as part of the engagement process.
The Company has monitoring procedures in place to identify and follow up on any overdue debts.
Credit risk from balances with banks and financial institutions is managed by the Company’s finance department in accordance with the Company’s policy to only place funds with approved counterparties with the appropriate credit rating.
The Company is exposed to no material credit risk.
Liquidity risk
Liquidity risk is the risk that necessary sources of funding for the Company’s business activities may not be available.
The Company manages liquidity risk by maintaining adequate reserves, banking facilities and reserve borrowing facilities, by continuously monitoring forecast and actual cash flows, and by matching the maturity profiles of financial assets and liabilities.
The Company is utilizing shareholder funds, collaboration agreements, grant funding and asset finance to support its working capital requirements.
All cash funds are held with a maturity of three months or less.
Market risk
Market risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market prices. Market risk comprises three types of risk: interest rate risk, currency risk and other price risk, such as equity price risk and commodity risk.
Interest rate risk
Interest rate risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market interest rates. The Company is exposed to no material interest rate risk.
Currency risk
The Group has transactions denominated in various currencies, with the principal currency exposure being fluctuations in the U.S. dollar and euros against pound sterling. The Group’s exposure to the risk of changes in foreign exchange rates relates primarily to the Group’s Convertible Loan Notes that are denominated in US Dollars and a limited number of supplier agreements denominated in currencies other than pound sterling. As at December 31, 2021, a 1% increase in the value of the US dollar against pound sterling would reduce the liability for the Convertible Loan Notes by £67,388. As at December 31, 2021, a 1% decrease in the value of the US dollar against pound sterling would increase the liability for the Convertible Loan Notes by £68,750.
Equity price risk
The Convertible Loan Notes issued by the Group contain an embedded derivative component that is accounted for at fair value at each period end. A change in the estimated underlying price per share will impact on the valuation of the embedded derivative. As at December 31, 2021, a 5% increase in the estimated share price would increase the value of the embedded derivative by £ 1,065,684 and a 5% decrease in the estimated share price would increase the value of the embedded derivative by £1,055,358.
| Item 12. | Description of Securities other than Equity Securities |
| A. | Debt Securities |
Not applicable.
| 149 |
| B. | Warrants and Rights |
See description of our publicly traded warrants in Item 10.B.
| C. | Other Securities |
Not applicable.
| D. | American Depositary Shares |
See description of our American Depositary Shares, or our ADSs, in Item 10.B.
PART II
| Item 13. | Defaults, Dividend Arrearages and Delinquencies |
None.
| Item 14. | Material Modifications to the Rights of Security Holders and Use of Proceeds |
None.
| Item 15. | Controls and Procedures |
| A. | Disclosure Controls and Procedures |
We maintain “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended, or the Exchange Act, that are designed to ensure that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms, and is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure. Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Exchange Act Rules 13a-15(e) and 15d-15(e)) as of December 31, 2021. In conducting its assessment of internal control over financial reporting, management based its evaluation on the Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on such evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that, as of December 31, 2021, our disclosure controls and procedures were effective.
| B. | Managements Annual Report on Internal Control over Financial Reporting |
This Annual Report does not include a report of management’s assessment regarding internal control over financial reporting due to a transition period established by rules of the Securities and Exchange Commission for newly public companies.
| C. | Attestation Report of the Registered Public Accounting Firm |
This report does not include an attestation report of our registered public accounting firm as we are an emerging growth company as defined in Section 2(a) of the Securities Act.
| D. | Changes in Internal Control Over Financial Reporting |
There has been no change in our internal control over financial reporting (as defined in Rule 13a-15(f) under the Exchange Act) that occurred during the period covered by this Annual Report that has materially affected, or is reasonably likely to materially affect, internal control over financial reporting.
| 150 |
| Item 16A. | Audit Committee Financial Expert |
The audit committee consists of James Culverwell (chair), Arlene Morris and Edward Niemczyk. The audit committee consists exclusively of members of our board who are financially literate, and our board of directors has determined that James Culverwell is an “audit committee financial expert” as defined by applicable SEC rules and has the requisite financial sophistication as defined under the applicable Nasdaq rules and regulations. Mr. Culverwell is independent as such term is defined in Rule 10A-3 under the Exchange Act and under the listing standards of the Nasdaq Stock Market.
| Item 16B. | Code of Ethics |
We have adopted a Code of Business Conduct and Ethics, or Code of Ethics, applicable to our employees, senior management, and directors, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. A current copy of the Code of Ethics is posted on our website, which is located at www.tcbiopharm.com. Information contained on, or that can be accessed through, our website does not constitute a part of this Annual Report and is not incorporated by reference herein.
| Item 16C. | Principal Accountant Fees and Services |
Our financial statements have been prepared in accordance with IFRS and are audited by Ernst & Young LLP, our independent registered public accounting firm registered with the Public Company Accounting Oversight Board in the United States.
Ernst & Young LLP has served as our independent registered public accountant for each of the years ended December 31, 2020 and December 31, 2021, for which audited statements appear in this Annual Report.
The following table shows the aggregate fees billed to us, including some of our subsidiaries, for services rendered by Ernst & Young LLP.
| Year ended December 31, | ||||||||
| 2020 | 2021 | |||||||
| (in thousands) | ||||||||
| Audit Fees | £ | 116 | £ | 125 | ||||
| Audit-Related Fees (1) | 58 | 309 | ||||||
| Total | £ | 174 | £ | 434 | ||||
| (1) | Audit-Related Fees are primarily for quarterly reviews and services related to SEC filings, including comfort letters, consents and comment letters. |
Our Audit Committee reviews and pre-approves the scope and the cost of audit services related to us and permissible non-audit services performed by the independent auditors, other than those for de minimis services which are approved by the Audit Committee prior to the completion of the audit. All of the services related to our company provided by Ernst & Young LLP during the last two fiscal years have been approved by the Audit Committee after February 2022, and prior to February 2022 by the board of directors.
| 151 |
| Item 16D. | Exemptions From the Listing Standards for Audit Committee |
Not applicable.
| Item 16E. | Purchasers of Equity Securities by the Issuer and Affiliated Purchasers |
Not applicable.
| Item 16F. | Change in the Registrant’s Certifying Accountant |
None.
| Item 16G | Corporate Governance |
See Item 6.B., where the exemptions provided to foreign private issuers by the Nasdaq Listing Rules that we take advantage of are discussed.
| Item 16H. | Mine Safety Disclosure |
Not applicable.
| Item 16I. | Disclosure Regarding Foreign Jurisdictions that Prevent Inspections |
None.
Part III
| Item 17 | Financial Statements |
We have elected to provide financial statements pursuant to Item 18.
| Item 18. | Financial Statements |
The financial statements are filed as part of this Annual Report beginning on page F-1.
| Item 19. | Exhibits |
| 152 |
| 4.6 | Convertible Loan Note, up to $20,000,000 in principal amount | F-1 | 333-260492 | 10.6 | 10/26/2022 | |||||
| 4.7 | Form of Lock Up Agreement of Pre-IPO Smaller Shareholders | F-1 | 333-260492 | 10.8 | 10/26/2022 | |||||
| 4.8 | Form of Lock Up Agreement of Pre-IPO Management and Larger Shareholders | F-1 | 333-260492 | 10.9 | 10/26/2022 | |||||
| 4.9 | Form of Lock Up Agreement of Holders of Convertible Loan Notes | F-1 | 333-260492 | 10.10 | 10/26/2022 | |||||
| 4.10* | Form of Deed of Indemnity for directors and officer | |||||||||
| 4,11* | Description of Securities of Registrant | |||||||||
| 4.12 | Code of Ethics of the Registrant | F-1 | 333-260492 | 11.1 | 10/26/2022 | |||||
| 8.1 | List of Subsidiaries of Registrant | F-1 | 333-260492 | 21.1 | 10/26/2022 | |||||
| 12.1* | Rule 13a-14(a)/15d-14(a) Certification of Chief Executive Officer, as adopted pursuant to §302 of the Sarbanes-Oxley Act of 2002. | |||||||||
| 12.2* | Rule 13a-14(a)/15d-14(a) Certification of Chief Financial Officer, as adopted pursuant to §302 of the Sarbanes-Oxley Act of 2002. | |||||||||
| 13.1* |
101.INS XBRL Instance Document
101.SCH XBRL Taxonomy Extension Schema Document
101.CAL XBRL Taxonomy Extension Calculation Linkbase Document
101.DEF XBRL Taxonomy Extension Definition Linkbase Document
101.LAB XBRL Taxonomy Extension Label Linkbase Document
101.PRE XBRL Taxonomy Extension Presentation Linkbase Document
| * | Filed herewith. |
| 153 |
SIGNATURE
The registrant hereby certifies that it meets all of the requirements for filing on Form 20-F and that it has duly caused and authorized the undersigned to sign this Annual Report on its behalf.
| TC BIOPHARM (HOLDINGS) PLC | ||
| By: | /s/ Bryan Kobel | |
| Name: | Bryan Kobel | |
| Title: | Chief Executive Officer | |
Date: May 13, 2022
| 154 |
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
| F-1 |
Report of Independent Registered Public Accounting Firm
To the Shareholders and the Board of Directors of TC BioPharm (Holdings) plc
Opinion on the Financial Statements
We have audited the accompanying consolidated statements of financial position of TC BioPharm (Holdings) plc (the Company) as of December 31, 2021 and 2020, the related consolidated statements of comprehensive loss, changes in equity and cash flows for each of the three years in the period ended December 31, 2021, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2021 and 2020, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2021, in conformity with International Financial Reporting Standards (IFRS) as issued by the International Accounting Standards Board (IASB).
The Company’s Ability to Continue as a Going Concern
The accompanying consolidated financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the financial statements, the Company has suffered recurring losses from operations, has a working capital deficiency, and has stated that substantial doubt exists about the Company’s ability to continue as a going concern. Management’s evaluation of the events and conditions and management’s plans regarding these matters are also described in Note 1. The consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
| /s/ |
|
| We have served as the Company’s auditor since 2019. | |
| May 13, 2022 |
| F-2 |
TC BIOPHARM (HOLDINGS) PLC
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
FOR THE YEARS ENDED DECEMBER 31, 2021
| 2021 | 2020 | 2019 | ||||||||||||||
| Notes | £ | £ | £ | |||||||||||||
| Revenue | 3 | |||||||||||||||
| Research and development expenses | ( | ) | ( | ) | ( | ) | ||||||||||
| Administrative expenses | ( | ) | ( | ) | ( | ) | ||||||||||
| Administrative expenses – costs related to listing | ( | ) | - | - | ||||||||||||
| Foreign exchange losses | ( | ) | - | - | ||||||||||||
| Other income | 4 | |||||||||||||||
| Total operating expenses, net | ( | ) | ( | ) | ( | ) | ||||||||||
| Change in fair value of convertible loan derivatives | ( | ) | - | - | ||||||||||||
| Finance income | ||||||||||||||||
| Finance costs | 6 | ( | ) | ( | ) | ( | ) | |||||||||
| Loss before tax | 5 | ( | ) | ( | ) | ( | ) | |||||||||
| Income tax credit | 7 | |||||||||||||||
| Net loss for the year and Total comprehensive loss | ( | ) | ( | ) | ( | ) | ||||||||||
| Basic and diluted loss per share | 9 | ( | ) | ( | ) | ( | ) | |||||||||
The accompanying notes form an integral part of these consolidated financial statements.
| F-3 |
TC BIOPHARM (HOLDINGS) PLC
CONSOLIDATED STATEMENTS OF FINANCIAL POSITION
AS AT,
December 31, 2021 | December 31, 2020 | |||||||||||
| (Adjusted) | ||||||||||||
| Notes | £ | £ | ||||||||||
| Assets | ||||||||||||
| Non-current assets | ||||||||||||
| Intangible assets | 10 | |||||||||||
| Right of use assets | 15 | |||||||||||
| Property, plant and equipment | 11 | |||||||||||
| Total non-current assets | ||||||||||||
| Current assets | ||||||||||||
| Trade and other receivables | 12 | |||||||||||
| Corporation tax receivable | ||||||||||||
| Cash and cash equivalents | ||||||||||||
| Total current assets | ||||||||||||
| Total assets | ||||||||||||
| Equity | ||||||||||||
| Share capital | 18 | |||||||||||
| Accumulated deficit | ( | ) | ( | ) | ||||||||
| Other reserves | 18 | |||||||||||
| Total equity | ( | ) | ( | ) | ||||||||
| Non-current liabilities | ||||||||||||
| Deferred income | 16 | |||||||||||
| Lease liabilities and similar | 15 | |||||||||||
| Total non-current liabilities | ||||||||||||
| Current liabilities | ||||||||||||
| Deferred income | 16 | |||||||||||
| Trade and other payables | 13 | |||||||||||
| Convertible loan derivatives | 14 | - | ||||||||||
| Convertible loan | 14 | - | ||||||||||
| Lease liabilities and similar | 15 | |||||||||||
| Total current liabilities | ||||||||||||
| Total liabilities | ||||||||||||
| Total equity and liabilities | ||||||||||||
Share capital, Share premium and Other reserves in the table above have been adjusted to give retrospective effect to the Group’s corporate reorganization. Further details of the effects of this reorganization are provided in Note 18 to these consolidated financial statements. The effect of these reclassifications has had no impact on Total equity or the Accumulated deficit.
The accompanying notes form an integral part of these consolidated financial statements.
| F-4 |
TC BIOPHARM (HOLDINGS) PLC
CONSOLIDATED STATEMENTS OF CHANGES IN EQUITY
FOR THE YEARS ENDED,
| Share capital – adjusted | Accumulated deficit | Other reserves - adjusted | Total equity | |||||||||||||||||
| Notes | £ | £ | £ | £ | ||||||||||||||||
| As at January 1, 2019 - adjusted | ( | ) | ( | ) | ||||||||||||||||
| Net loss for the year and Total comprehensive loss | ( | ) | - | ( | ) | |||||||||||||||
| Recognition of share-based payment costs | 19 | - | ||||||||||||||||||
| Issue of share capital, net of issuance costs | 18 | |||||||||||||||||||
| As at December 31, 2019 | ( | ) | ( | ) | ||||||||||||||||
| As at January 1, 2020 | ( | ) | ( | ) | ||||||||||||||||
| Net loss for the year and Total comprehensive loss | ( | ) | - | ( | ) | |||||||||||||||
| Recognition of share-based payment costs | 19 | - | ||||||||||||||||||
| Issue of share capital, net of issuance costs | 18 | |||||||||||||||||||
| As at December 31, 2020 | ( | ) | ( | ) | ||||||||||||||||
| As at January 1, 2021 | ( | ) | ( | ) | ||||||||||||||||
| Net loss for the year and Total comprehensive loss | - | ( | ) | - | ( | ) | ||||||||||||||
| Issue of share capital, net of issuance costs | 18 | - | ||||||||||||||||||
| As at December 31, 2021 | ( | ) | ( | ) | ||||||||||||||||
Share capital, Share premium and Other reserves in the table above have been adjusted to give retrospective effect to the Group’s corporate reorganization. Further details of the effects of this reorganization are provided in Note 18. The accompanying notes form an integral part of these financial statements.
| F-5 |
TC BIOPHARM (HOLDINGS) PLC
CONSOLIDATED CASH FLOW STATEMENT
FOR THE YEARS ENDED DECEMBER 31, 2021
2021 | 2020 | 2019 | ||||||||||||||
| Notes | £ | £ | £ | |||||||||||||
| Cash flows from operating activities | ||||||||||||||||
| Loss before tax | ( | ) | ( | ) | ( | ) | ||||||||||
| Adjustments for: | ||||||||||||||||
| Depreciation | ||||||||||||||||
| Amortization of intangible assets | ||||||||||||||||
| Amortization of right of use assets | ||||||||||||||||
| Share-based payment expense | - | |||||||||||||||
| Change in fair value of convertible loan derivatives | - | - | ||||||||||||||
| Net foreign exchange losses | ||||||||||||||||
| Finance income | ( | ) | ( | ) | ( | ) | ||||||||||
| Finance costs | ||||||||||||||||
| Loss on disposal of intangible assets | - | |||||||||||||||
| Movements in working capital: | ||||||||||||||||
| Decrease in deferred income | ( | ) | ( | ) | ( | ) | ||||||||||
| (Increase)/decrease in trade and other receivables | ( | ) | ||||||||||||||
| Increase/(decrease) in trade and other payables | ( | ) | ||||||||||||||
| Cash used in operations | ( | ) | ( | ) | ( | ) | ||||||||||
| Interest paid | ( | ) | ( | ) | ( | ) | ||||||||||
| Interest received | ||||||||||||||||
| Income tax received / (paid) | ( | ) | ||||||||||||||
| Net cash flows used in operating activities | ( | ) | ( | ) | ( | ) | ||||||||||
| Cash flows from investing activities | ||||||||||||||||
| Purchase of property, plant and equipment | ( | ) | ( | ) | ( | ) | ||||||||||
| Purchase of intangible assets | ( | ) | ( | ) | ( | ) | ||||||||||
| Net cash flows used in investing activities | ( | ) | ( | ) | ( | ) | ||||||||||
| Cash flows from financing activities | ||||||||||||||||
| Repayment of lease liabilities | ( | ) | ( | ) | ( | ) | ||||||||||
| Receipt from issuance of convertible loan (net of issue costs) | 14 | - | - | |||||||||||||
| Receipt of sale and leaseback asset finance | - | - | ||||||||||||||
| Proceeds received on issue of shares | ||||||||||||||||
| Share issue costs | ( | ) | ( | ) | - | |||||||||||
| Net cash flows from financing activities | ||||||||||||||||
| Net increase/(decrease) in cash and cash equivalents | ( | ) | ( | ) | ||||||||||||
| Foreign exchange movements on cash and cash equivalents | ( | ) | ( | ) | ||||||||||||
| Cash and cash equivalents at the beginning of the year | ||||||||||||||||
| Cash and cash equivalents at the end of the year | 21 | |||||||||||||||
The accompanying notes form an integral part of these consolidated financial statements.
| F-6 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
| 1. | Accounting policies |
General information
TC BioPharm (Holdings) plc (“TC BioPharm” or the “Company”) is incorporated as a Public limited company, limited by shares, in Scotland and domiciled in the United Kingdom (registration number: SC713098) and has the following wholly owned subsidiaries TC BioPharm Limited, TC BioPharm (North America) Inc. and TC BioPharm BV (together the “Group”). The registered office is: Maxim 1, 2 Parklands Way, Holytown, Motherwell, Lanarkshire, Scotland, ML1 4WR.
The principal activity of the Group is as a clinical stage immuno-therapy company pioneering commercialization of allogeneic, ‘off-the-shelf’ gamma-delta T cell (‘GD-T’) therapies, ranging from unmodified GD-T therapies to treat haematological cancers and viral infections, to sophisticated proprietary GD-T CAR-T products designed to reach and treat solid tumors.
TC BioPharm (Holdings) plc was incorporated on October 25, 2021. On December 17, 2021, all shareholders in TC BioPharm Limited and holders of convertible loan notes in TC BioPharm Limited exchanged their shares and convertible loan notes for the same number and classes of newly issued shares and/or convertible loan notes in TC BioPharm (Holdings) plc and, as a result, TC BioPharm Limited became a wholly owned subsidiary of TC BioPharm (Holdings) plc. The corporate reorganization has been accounted for as a business combination under common control and therefore, TC BioPharm (Holdings) plc is a continuation of TC BioPharm Limited and its subsidiaries. The corporate reorganization has been given retrospective effect in these consolidated financial statements, which represent the consolidated financial statements of TC BioPharm (Holdings) plc. All TC BioPharm Limited share options granted to directors and employees under share option plans that were in existence immediately prior to the reorganization were exchanged for share options in TC BioPharm (Holdings) plc on a one-for-one basis with no change in any of the terms or conditions.
On December 17, 2021 and subsequent to the group reorganization, the Company undertook a share split such that one issued ordinary share was exchanged for ten new ordinary shares. As a result of the share split, all references in these consolidated financial statements and accompanying notes to units of ordinary shares or per share amounts are reflective of the forward share split for all periods presented. In addition, the exercise prices and the numbers of ordinary shares issuable upon the exercise of any outstanding options to purchase ordinary shares were proportionally adjusted pursuant to the respective anti-dilution terms of the share-based payment plans.
Basis of preparation
The principal accounting policies applied in the preparation of these consolidated financial statements are set out below.
The consolidated financial statements have been prepared in accordance with International Financial Reporting Standards (“IFRS”) as issued by the International Accounting Standards Board (“IASB”).
The Company’s functional currency is the pound sterling. The Group’s presentational currency is the pound sterling. Monetary amounts in these consolidated financial statements are rounded to the nearest pound.
Consolidation of a subsidiary begins when the Group obtains control over the subsidiary and ceases when the Group loses control of the subsidiary. Where necessary, adjustments are made to the financial statements of subsidiaries to bring the accounting policies in line with those used by the Group. All intra-group transactions, balances, equity, income and expenses are eliminated on consolidation.
Share capital, share premium and other reserves have been adjusted to give retrospective effect to the Group’s corporate reorganization. Further details of the effects of this reorganization are provided in Note 18. The accompanying notes form an integral part of these financial statements.
These consolidated financial statements were authorized by the Board of Directors on May 13, 2022.
| F-7 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
The Company has the following interests in subsidiary undertakings:
| Name | Country of incorporation |
Holding |
Proportion held | Nature of business | ||||
Going concern
The Company was incorporated in 2014 to develop therapeutic products based around its gamma delta T cell platform technology, with the objective of conducting clinical trials to demonstrate safety and efficacy and eventually being granted regulatory approval to market and sell its products. This activity was expected to be ongoing over several years and has involved considerable expenditure to date on carrying out research and development and conducting clinical trials. In common with most development and/or clinical stage biotechnology companies, the Company has not yet generated any revenues from sales of products, but has obtained cash to finance its research, development and clinical trial activities from equity, debt and grant financings and from receipts from partners under collaborative co-development agreements. The Company is expected to stay in this clinical development stage for several years before any product becomes marketable. The Company therefore expects to continue to incur significant losses in the foreseeable future,
As
at December 31, 2021, the Company had an accumulated deficit of £
As
at December 31, 2021, the Company’s cash and cash equivalents amounted to £
In
February 2022 the Company raised $
The
Company received $
On
April 30, 2022, the Company had cash on hand of $
| F-8 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
In common with many early-stage biotechnology companies our future liquidity needs, and ability to address them, will largely be determined by the availability of capital, both generally and in particular to fund our product candidates and key development and regulatory projects. We anticipate having to raise capital routinely on the capital markets, taking advantage of our public listing. We are currently progressing various cash accretive initiatives to fill the gap in short-term working capital referred to above, which could be in the form of an equity raise or other forms of financings such as collaborations or licensing arrangements.
We believe that these initiatives should improve our net short-term working capital position sufficiently to provide sufficient capital to finance planned operations into early 2023, and, before then, we would expect to be in a position to raise significantly greater capital to fund our longer-term plan. However, there can be no certainty that these initiatives will be successful and, if they are not, management will seek to deploy alternative plans, which could have a potentially significant negative impact on shareholder and asset value. Such plans could include all or any of the following: raising additional capital through low priced and/or complex equity and/or debt financings; entering transactions involving sales, joint venturing or licensing of intellectual property; reducing and/or deferring discretionary spending on research and development or clinical programs; restructuring our operating model to take advantage of our manufacturing capability to generate short term revenues; reducing our cash burn rate through reduction in planned operating costs. The accompanying consolidated financial statements have been prepared in conformity with IFRS as issued by IASB, which contemplate continuation of the Company as a going concern (having adequate working capital to maintain operations through the Going Concern Period). The Company has not established a source of revenues sufficient to cover its operating costs, and as such, has been dependent on funding operations primarily through the sale of securities, commercial partnerships, and/or grants. The Company expects to incur further losses over the next several years as it develops its clinical products towards the market. The Company has spent, and expects to continue to spend, substantial amounts of funding to implement its business strategy. Although the completion of its IPO on Nasdaq was a major milestone for the Company, as it opens much wider avenues to raise future finance, the market conditions were such that the offering raised less than was initially targeted, and the proceeds of the offering alone are not adequate to finance the Company’s clinical and product development programs through the Going Concern Period. Nonetheless the proceeds of the offering, together with the anticipated proceeds from various initiatives referred to above, cause management to believe that the Company will have sufficient liquidity to fund its operations through the Going Concern Period, and, on that basis management continues to view the Company as a going concern.
Notwithstanding this, management recognizes, that there is considerable risk in both (i) the ability of the Company to implement successfully the short term working capital that it requires to maintain operations through the Going Concern Period, referred to above, or otherwise; and (ii) the nature of the early stage clinical development and research and development activities that it is undertaking, where, by definition , there can be no assurance that it was be able to bring any of its proposed products to market. If the Company is unable to maintain adequate liquidity, future operations will need to be scaled back or discontinued. These conditions raise substantial doubt about the Company’s ability to continue as a going concern. The Company’s consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
| F-9 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Revenue – collaboration agreements
Revenue is recognized on upfront collaboration payments on a straight-line basis over the estimated term over which the services promised will be provided.
The business is entitled to receive contractual milestone payments on achievement of certain performance obligations and these are recognized when the milestones are certain to occur.
Refer to Note 3 – Critical accounting estimates and judgements for further discussion on revenue from contracts with customers.
Segment reporting
The
Group operates in
Research & Development
Research expenditure is expensed in the year in which it is incurred. Identifiable development expenditure is capitalized to the extent that the technical, commercial and financial feasibility can be demonstrated. We have not capitalized any development expenditures since inception.
Grants
Grants are recognized when it is reasonable to expect that the grants will be received and that all related conditions will be met, usually on submission of a valid claim for payment. Revenue grants are treated as deferred income and are credited to the consolidated statements of comprehensive loss to match against the expenditure towards which they are intended to contribute. Government support received under the Coronavirus Job Retention Scheme is recognized in the month of submission of the claim.
Income tax
Any tax currently payable is based on taxable profit for the period. Taxable profit differs from net profit as reported in the profit or loss because it excludes items of income or expense that are taxable or deductible in other years and it further excludes items that are never taxable or deductible. The Group’s liability for current tax is calculated using tax rates that have been enacted or substantively enacted by the reporting end date.
Deferred tax
Deferred tax is the tax expected to be payable or recoverable on differences between the carrying amounts of assets and liabilities in the financial statements and the corresponding tax bases used in the computation of taxable profit/loss, and is accounted for using the balance sheet liability method. Deferred tax liabilities are generally recognized for all taxable temporary differences and deferred tax assets are recognized to the extent that it is probable that taxable profits will be available against which deductible temporary differences can be utilized. Such assets and liabilities are not recognized if the temporary difference arises from goodwill or from the initial recognition of other assets and liabilities in a transaction that affects neither the tax profit nor the accounting profit.
| F-10 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Deferred tax (continued)
The carrying amount of deferred tax assets is reviewed at each reporting end date and reduced to the extent that it is no longer probable that sufficient taxable profits will be available to allow all or part of the asset to be recovered. Deferred tax is calculated at the tax rates that are expected to apply in the period when the liability is settled or the asset is realized. Deferred tax is charged or credited in the profit or loss, except when it relates to items charged or credited directly to equity, in which case the deferred tax is also dealt with in equity. Deferred tax assets and liabilities are offset when the Group has a legally enforceable right to offset current tax assets and liabilities and the deferred tax assets and liabilities relate to taxes levied by the same tax authority.
Income tax credit
The
Group carries out extensive research and development activities, where we benefit from the UK research and development tax relief and
expenditure credit regimes. We are able to surrender some of our income tax losses for a cash rebate of up to
Employee benefits
The Group operates a defined contribution scheme for the benefit of its employees. Contributions payable are charged to the profit or loss in the year they are payable.
Property, plant and equipment
Property, plant and equipment relates to computer equipment, facility and scientific equipment and office equipment which are initially recorded at cost. They are subsequently stated at historical cost less accumulated depreciation and impairment losses. Historical cost includes expenditure that is directly attributable to the acquisition of the items and bringing them into their intended use.
Property, plant and equipment is derecognized on disposal or when no future economic benefits are expected from their use or disposal. Gains or losses arising from de-recognition represent the difference between the net disposal proceeds, if any, and the carrying amount, and are included in the statements of comprehensive loss in the period of de-recognition.
Depreciation is provided at rates intended to write down the cost of the assets over their expected useful lives, as follows;
| Facility & scientific equipment | - |
| Computer equipment | - |
| Office equipment | - |
All depreciation rates are applied on a straight-line basis.
Intangible assets
Intangible assets relate to software, patents and licences. Intangible assets are recognized where it is probable that there will be a future economic benefit and that this can be reliably measured.
Software
represents the historical cost of installation of third-party software used within the Group to maintain and control the Group’s
quality system. The software is hosted and controlled on the Group’s servers and can be used independently of the related hardware.
| F-11 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Intangible assets (continued)
Patent
costs represent the costs of securing patents in relation to the Group’s intellectual property. Patent costs are amortized, on
a straight-line basis, over the remaining legal life of the relevant patents (the average estimated patent life is
License
costs represent costs incurred for securing use of third-party technology. License costs are amortized, on a straight-line basis, over
the life of the relevant license (
Impairment of tangible and intangible assets
The Group reviews the carrying amounts of its tangible and intangible assets where there is any indication that those assets have suffered an impairment loss. If any such indication exists, the recoverable amount of the asset is estimated in order to determine the extent of the impairment loss (if any). The recoverable amount is determined for an individual asset, unless the asset does not generate cash inflows that are largely independent of those from other assets or groups of assets in which case the Group estimates the recoverable amount of the cash-generating unit to which the asset belongs.
Recoverable amount is the higher of fair value less costs to sell and value-in-use. In assessing value-in-use, the estimated future cash flows are discounted to their present value using a pre-tax discount rate that reflects current market assessments of the time value of money and the risks specific to the asset for which the estimates of future cash flows have not been adjusted.
If the recoverable amount of an asset (or cash-generating unit) is estimated to be less than its carrying amount, the carrying amount of the asset (or cash-generating unit) is reduced to its recoverable amount. An impairment loss is recognized immediately in profit or loss.
Cash and cash equivalents
Cash and cash equivalents include cash on hand, deposits held on call with banks and other short-term liquid investments with maturities of three months or less.
Financial assets
Initial recognition and measurement
Financial assets are classified, at initial recognition, and subsequently measured at amortized cost, fair value through other comprehensive income (OCI), and fair value through profit or loss.
The classification of financial assets at initial recognition depends on the financial asset’s contractual cash flow characteristics and the Group’s business model for managing them. With the exception of trade receivables that do not contain a significant financing component, the Group initially measures a financial asset at its fair value plus, in the case of a financial asset not at fair value through profit or loss, transaction costs. Trade receivables that do not contain a significant financing component are measured at the transaction price determined under IFRS 15.
In order for a financial asset to be classified and measured at amortized cost or fair value through OCI, it needs to give rise to cash flows that are ‘solely payments of principal and interest (SPPI)’ on the principal amount outstanding. This assessment is referred to as the SPPI test and is performed at an instrument level.
| F-12 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Financial assets (continued)
The Group’s business model for managing financial assets refers to how it manages its financial assets in order to generate cash flows. The business model determines whether cash flows will result from collecting contractual cash flows, selling the financial assets, or both.
Financial assets at amortized cost
The Group measures financial assets at amortized cost if both of the following conditions are met:
| ● | The financial asset is held within a business model with the objective to hold financial assets in order to collect contractual cash flows; and | |
| ● | The contractual terms of the financial asset give rise on specified dates to cash flows that are solely payments of principal and interest on the principal amount outstanding. |
Financial assets at amortized cost are subsequently measured using the effective interest (EIR) method and are subject to impairment. Gains and losses are recognized in consolidated statements of comprehensive loss when the asset is derecognized, modified or impaired.
The Group’s financial assets measured at amortized cost includes trade and other receivables.
Financial assets are recognized in the Group’s consolidated statement of financial position when the Group becomes party to the contractual provisions of the instrument.
Financial assets are classified into specified categories. The classification depends on the nature and purpose of the financial assets and is determined at the time of recognition.
Financial assets are initially measured at fair value plus transaction costs, other than those classified as fair value through profit and loss, which are measured at fair value.
Derecognition
A financial asset (or, where applicable, a part of a financial asset or part of a group of similar financial assets) is primarily derecognized (i.e. removed from the Group’s consolidated statement of financial position) when:
| ● | The rights to receive cash flows from the asset have expired; or | |
| ● | The Group has transferred its rights to receive cash flows from the asset or has assumed an obligation to pay the received cash flows in full without material delay to a third party under a ‘pass-through’ arrangement; and either (a) the Group has transferred substantially all the risks and rewards of the asset, or (b) the Group has neither transferred nor retained substantially all the risks and rewards of the asset, but has transferred control of the asset. |
When the Group has transferred its rights to receive cash flows from an asset or has entered into a pass-through arrangement, it evaluates if, and to what extent, it has retained the risks and rewards of ownership. When it has neither transferred nor retained substantially all of the risks and rewards of the asset, nor transferred control of the asset, the Group continues to recognize the transferred asset to the extent of its continuing involvement. In that case, the Group also recognizes an associated liability. The transferred asset and the associated liability are measured on a basis that reflects the rights and obligations that the Group has retained.
Continuing involvement that takes the form of a guarantee over the transferred asset is measured at the lower of the original carrying amount of the asset and the maximum amount of consideration that the Group could be required to repay.
| F-13 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Financial assets (continued)
Impairment of financial assets
The Group recognizes an allowance for expected credit losses (ECLs) for all debt instruments not held at fair value through profit or loss. ECLs are based on the difference between the contractual cash flows due in accordance with the contract and all the cash flows that the Group expects to receive, discounted at an approximation of the original effective interest rate. The expected cash flows will include cash flows from the sale of collateral held or other credit enhancements that are integral to the contractual terms. ECLs are recognized in two stages. For credit exposures for which there has not been a significant increase in credit risk since initial recognition, ECLs are provided for credit losses that result from default events that are possible within the next 12-months (a 12-month ECL). For those credit exposures for which there has been a significant increase in credit risk since initial recognition, a loss allowance is required for credit losses expected over the remaining life of the exposure, irrespective of the timing of the default (a lifetime ECL). For trade receivables and contract assets, the Group applies a simplified approach in calculating ECLs. Therefore, the Group does not track changes in credit risk, but instead recognizes a loss allowance based on lifetime ECLs at each reporting date. The Group has established a provision matrix that is based on its historical credit loss experience, adjusted for forward-looking factors specific to the debtors and the economic environment.
Financial liabilities
Initial recognition and measurement
Classification as debt or equity
A financial instrument issued by the Group is classified as either financial liabilities or as equity in accordance with the substance of the contractual arrangements and the definitions of a financial liability and an equity instrument.
Equity instruments
An equity instrument is any contract that evidences a residual interest in the assets of an entity after deducting all of its liabilities. Equity instruments issued by the Group are recognised at the proceeds received, net of direct issue costs.
Repurchase of the Company’s own equity instruments is recognised and deducted directly in equity. No gain or loss is recognised in profit or loss on the purchase, sale, issue or cancellation of the Company’s own equity instruments.
Compound instruments
The component parts of a financial instrument issued by the Group are classified separately as financial liabilities and equity in accordance with the substance of the contractual arrangements and the definitions of a financial liability and an equity instrument. A conversion option that will be settled by the exchange of a fixed amount of cash or another financial asset for a fixed number of the Company’s own equity instruments is an equity instrument. In absence of this characteristic, a conversion option is classified as an embedded derivative liability.
At the date of issue, the fair value of the liability component is estimated using the prevailing market interest rate for a similar non-convertible instrument. This amount is recorded as a liability on an amortised cost basis using the effective interest method until extinguished upon conversion or at the instrument’s maturity date.
The conversion option classified as equity is determined by deducting the amount of the liability component from the issue proceeds of the compound instrument as a whole. This is recognised and included in equity, net of income tax effects, and is not subsequently remeasured. In addition, the conversion option classified as equity will remain in equity until the conversion option is exercised, in which case the balance recognised in equity will be transferred to another equity caption. Where the conversion option remains unexercised at the maturity date of the convertible loan note, the balance recognised in equity will be transferred to another equity caption. No gain or loss is recognised in profit or loss upon conversion or expiration of the conversion option.
| F-14 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Transaction costs that relate to the issue of the convertible loan notes are allocated to the liability and equity components in proportion to the allocation of the gross proceeds. Transaction costs relating to the equity component are recognised directly in equity. Transaction costs relating to the liability component are included in the carrying amount of the liability component and are amortised over the lives of the convertible loan notes using the effective interest method.
Embedded derivatives
An embedded derivative is a component of a hybrid contract that also includes a non-derivative host – with the effect that some of the cash flows of the combined instrument vary in a way similar to a stand-alone derivative.
Derivatives embedded in hybrid contracts with a financial asset host within the scope of IFRS 9 are not separated. The entire hybrid contract is classified and subsequently measured as either amortised cost or fair value as appropriate.
Derivatives embedded in hybrid contracts with hosts that are not financial assets within the scope of IFRS 9 (e.g. financial liabilities) are treated as separate derivatives when they meet the definition of a derivative, their risks and characteristics are not closely related to those of the host contracts and the host contracts are not measured at FVTPL.
If the hybrid contract is a quoted financial liability, instead of separating the embedded derivative, the Group generally designates the whole hybrid contract at FVTPL.
An embedded derivative is presented as a non-current asset or non-current liability if the remaining maturity of the hybrid instrument to which the embedded derivative relates is more than 12 months and is not expected to be realised or settled within 12 months.
Financial liabilities are classified, at initial recognition, as financial liabilities at fair value through profit or loss, loans and borrowings, payables, or as derivatives designated as hedging instruments in an effective hedge, as appropriate.
All financial liabilities are recognized initially at fair value and, in the case of loans and borrowings and payables, net of directly attributable transaction costs. The Group’s financial liabilities include trade and other payables, convertible loans and sale and lease back arrangements.
Derecognition
A financial liability is derecognized when the obligation under the liability is discharged or cancelled or expires. When an existing financial liability is replaced by another from the same lender on substantially different terms, or the terms of an existing liability are substantially modified, such an exchange or modification is treated as the derecognition of the original liability and the recognition of a new liability. The difference in the respective carrying amounts is recognized in the statement of profit or loss.
| F-15 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Leases
The Group reviews contracts to determine if a contract meets the definition of a lease. This means that the Group has the right to control the use of an identifiable asset for a period of time in exchange for consideration.
All leases are accounted for by recognizing a right-of-use asset and a lease liability except for:
| ● | Leases of low value assets; and | |
| ● | Leases with a duration of twelve months or less. |
Lease liabilities are measured at the present value of the contractual payments due to the lessor over the lease term, with the discount rate determined by reference to the rate inherent in the lease unless (as is typically the case) this is not readily determinable, in which case the Group’s incremental borrowing rate on commencement of the lease is used. Variable lease payments are only included in the measurement of the lease liability if they depend on an index or rate. In such cases, the initial measurement of the lease liability assumes the variable element will remain unchanged throughout the lease term. Other variable lease payments are expensed in the period to which they relate.
On initial recognition, the carrying value of the lease liability also includes:
| ● | Amounts expected to be payable under any residual value guarantee; | |
| ● | The exercise price of any purchase option granted in favor of the Group if it is reasonably certain to assess that option; | |
| ● | Any penalties payable for terminating the lease, if the term of the lease has been estimated on the basis of the termination option being exercised. |
Right-of-use assets are initially measured at the amount of the lease liability, reduced for any lease incentives received, and increased for:
| ● | Lease payments made at or before commencement of the lease; | |
| ● | Initial direct costs incurred; and | |
| ● | The amount of any provision recognized where the Group is contractually required to dismantle, remove or restore the leased asset. |
Subsequent to initial measurement, lease liabilities increase as a result of interest charged at a constant rate on the balance outstanding and are reduced for lease payments made. Right-of-use assets are amortized on a straight-line basis over the remaining term of the lease or over the remaining economic life of the asset if, rarely, this is judged to be shorter than the lease term. The interest charged and the amortization are recognized within the consolidated statements of comprehensive loss.
| F-16 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Leases (continued)
When the Group revises its estimate of the term of any lease (because, for example, it re-assesses the probability of a lessee extension or termination option being exercised), it adjusts the carrying amount of the lease liability to reflect the payments to make over the revised term, which are discounted at the same discount rate that applied on lease commencement. The carrying value of lease liabilities is similarly revised when the variable element of future lease payments dependent on a rate or index is revised. In both cases an equivalent adjustment is made to the carrying value of the right-of-use asset, with the revised carrying amount being amortized over the remaining (revised) lease term.
When the Group extends the scope of the lease and the extension was not part of the original terms of the contract, this is considered to be a lease modification and is treated as a separate additional lease.
Initial public offering (IPO) related expenses
Incremental costs deemed to be incurred and directly attributable to the planned offering of securities were held as prepayments prior to being deducted from the related proceeds of the offering in due course. Costs that relate to the stock market listing or are otherwise not incremental and directly attributable to issuing new shares, are recorded as an expense in the statement of comprehensive loss. Costs that relate to both share issuance and listing are allocated between those functions on a rational and consistent basis. In the absence of a more specific basis for apportionment, an allocation of common costs based on the proportion of new shares issued to the total number of (new and existing) shares listed has been used.
Foreign currencies
Transactions in currencies other than pounds sterling are recorded at the rates of exchange prevailing at the dates of the transactions. At each reporting end date, monetary assets and liabilities that are denominated in foreign currencies are remeasured at the rates prevailing on the reporting end date. Gains and losses arising on remeasurement are included in the profit or loss for the period.
| F-17 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Equity instruments
Equity instruments are in the form of Ordinary and A Ordinary shares (further details are included in Note 18). Equity instruments issued by the Company are recorded at the proceeds received, net of direct issue costs. Costs that are not incremental and directly attributable to issuing new equity instruments are recorded as an expense in the consolidated statements of comprehensive loss.
Rights to subscribe for additional equity
Some investors have the right to subscribe for a fixed number of A Ordinary shares at an agreed share price at a future date upon the achievement of certain clinical and commercial milestones.
The value of the right to subscribe has been recognized as a derivative and classified within equity. The Company has adopted this accounting treatment as:
| ● | the value of the instrument will vary in response to changes in the underlying value of the A Ordinary shares, representing a derivative financial instrument | |
| ● | the right to subscribe is for a fixed number of shares at a fixed price, reflecting the definition of an equity instrument |
When considering the fair value of the right to subscribe for additional equity, the most appropriate basis to allocate value to payments was determined to be a Black Scholes Model, with reference to the nature of the contract award and future liquidity events. The fair value of these rights considers the following factors:
| ● | Exercise price | |
| ● | Current price of the underlying shares | |
| ● | Expected life of the award | |
| ● | Risk-free interest rate | |
| ● | Expected volatility | |
| ● | Expected dividend rate | |
| ● | Expected forfeiture rate |
| F-18 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 1. | Accounting policies (continued) |
Some employees, directors and consultants receive remuneration in the form of share-based payments as consideration for their services rendered. The fair value of equity-settled share-based payments to employees is determined at the date of grant and is expensed on a straight-line basis over the vesting period, with a corresponding increase in equity, based on the Group’s estimate of options that will eventually vest.
In respect of share-based payments to employees and directors, the estimated fair value of the options outstanding in the period was calculated by applying a Monte Carlo Simulation for those options issued in 2020 and a Black Scholes Model for those options issued in prior periods. The most appropriate approach is selected with reference to the share capital structure at the time of grant. In respect of the valuation for 2020, the Monte Carlo Simulation was deemed the most appropriate basis due to the preferential economic rights contained within equity issued in the year. When considering share-based payments to external consultants, the most appropriate basis to allocate value to payments was determined to be a Black Scholes Model, with reference to the nature of the contract award and future liquidity events. The fair value of share-based payments considers the following factors:
| ● | Exercise price | |
| ● | Current price of the underlying shares | |
| ● | Expected life of the award | |
| ● | Risk-free interest rate | |
| ● | Expected volatility | |
| ● | Expected forfeiture rate | |
| ● | Expected dividend rate |
Accounting Standards
In preparing these consolidated financial statements, the Group has applied all relevant IAS, IFRS and International Financial Reporting Interpretations Committee (“IFRIC”) Interpretations as of the date of approval of these consolidated financial statements and which are mandatory for the financial year ended December 31, 2021.
There have been no recent new accounting standards that have had a material impact on these consolidated financial statements and no new standards issued but not yet effective that are expected to have a material impact on the Group.
| F-19 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 2. | Critical accounting estimates and judgements |
In the application of the Group’s accounting policies, management are required to make judgements, estimates and assumptions about the carrying amount of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from these estimates.
The estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimate is revised where the revision affects only that period, or in the period of the revision and future periods where the revision affects both current and future periods.
Judgements made in applying accounting policies other than those involving estimations
Revenue from contracts with customers
Identification of contracts with pharma partners
The Group has entered into collaboration agreements with a number of parties. Application of IFRS 15 “Revenue from contracts and customers” on collaboration agreements requires judgement around whether these contracts were within the scope of IFRS 15.
The Group’s core business is around researching and developing immunotherapies and the contracts entered into with pharma partners are consistent with those objectives and the outputs are in line with the Group’s ordinary activities.
The contracts with pharma partners do not involve sharing the risks and benefits of a joint arrangement in the sense of IFRS 11 “Joint arrangements”.
In light of the nature of the work being undertaken with pharma partners, and the fact that these agreements have commercial substance with clearly defined milestones and rights and obligations for each party, management concluded that these collaboration agreements meet the definition of a contract with a customer and fall within the scope of IFRS 15.
Identification of performance obligations in contracts
The collaboration agreements entered into by the Group include obligations to fulfil the research and development programs. The Group identified, from reviews of the relevant agreements, that there are no specific obligations but an implied performance obligation to deliver each overall contracted research and development program. Reflecting the broad nature of these obligations, spanning the full duration of the contract, the obligations are satisfied over the expected duration of the relevant contract.
Determination and allocation of the transaction price
The collaboration agreements include a number of elements of consideration and are allocated to the satisfaction of the relevant obligation.
The Group can receive upfront payments as part of the consideration. The Group has determined that upfront payments are in connection with the performance of the research and development program and are satisfied during the duration of the contract.
The business is entitled to receive contractual milestone payments on achievement of certain performance obligations, with revenue being recognized in the same way. The relevant transaction price is allocated to the related milestone.
| F-20 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 2. | Critical accounting estimates and judgements (continued) |
Assumptions about the future and other sources of estimation uncertainty
Revenue from contracts with customers
Timing of revenue recognition
Revenue from upfront payments in connection with collaboration agreements is recognized over the estimated term over which the services promised will be provided. This term was estimated by management at the inception of each contract and evaluated at the year end. The estimated time to complete as at the year end is 23 months.
The
resulting deferred income liabilities are disclosed in Note 15. Due to the uncertainty around the time to complete multi-year collaboration
programs it is possible that the estimated terms may be extended. If the estimated term of the current contracts had been adjusted by
one year, then it would be expected that the corresponding revenue would have decreased by £
Valuation of ordinary shares
As there has been no public market for the Group’s ordinary shares until February 10, 2022, the estimated fair value of the ordinary shares has been determined by management, considering the most recently available third-party valuations of the Group’s ordinary shares, and the assessment of additional objective and subjective factors that it believed were relevant and which may have changed from the date of the most recent valuation through the date of the grant.
After considering the market approach, the income approach and the asset-based approach, we utilized the market approach to determine the estimated fair value of our ordinary shares based on its determination that this approach was most appropriate for a clinical-stage biopharmaceutical company at this point in its development, using the option-pricing method (“OPM”). Consideration was given to the American Institute of Certified Public Accountants’ Practice Aid: “Valuation of Privately-Held Company Equity Securities Issued as Compensation,” or the Practice Aid, in addition to input from management, the likelihood of completing an IPO and recent transactions with investors.
Following the Group’s IPO on February 10, 2022, which established a public trading market for our ordinary shares, it will no longer be necessary to estimate the fair value of our ordinary shares in connection with our accounting for share-based payment expenses, as the fair value of our ordinary shares will be determinable by reference to the trading price of our ordinary shares on Nasdaq.
Share option and other share-based payment assumptions
The determination of the value of share-based payments requires management to use professional expertise to arrive at assumptions to be used to calculate the value of the share-based payment. The estimated fair value of the options outstanding in the period was calculated by applying a Monte Carlo Simulation for those options issued in 2020 and a Black Scholes Model for those options issued in prior periods. The most appropriate approach is selected with reference to the share capital structure at the time of grant and the directors need to use judgement in setting the key assumptions. Further details are included in Note 19.
| F-21 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 2. | Critical accounting estimates and judgements (continued) |
The Company determines the share price used in the fair value calculation by reference to shares issued close to the time of grant of the share options. Consideration is given to the nature of the shares issued and investors in the rounds when evaluating the share price as well as an assessment of any factors that were relevant and which may have changed from the date of the most recent share issuance to the date of grant. As at December 31, 2021, as a privately held company, the Company’s share price does not have sufficient historical volatility to adequately assess the fair value of the share option grants. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that a volatility range of to was appropriate for the valuation of our share options.
The expected life of the option, beginning with the option grant date, was used in valuing our share options. The expected life used in the calculation of share-based payment expense is the time from the grant date to the expected exercise date. The life of the options, which is a subjective estimate that can materially alter the valuation, depends on the option expiration date, volatility of the underlying shares and vesting features.
IFRS 2 “Share-based Payment” requires the use of the risk-free rate of the country in which the entity’s shares are principally traded with a remaining term equal to the expected life of the option. This should also be the risk-free interest rate of the country in whose currency the exercise price is expressed. The Company has applied the appropriate risk-free rate, based on 4-year, 3-year and 2-year UK government bond yields as at the respective grant dates.
Convertible loan redemption date
The
Group calculates the effective interest rate (“EIR”) to consider the potential repayment at redemption date by reference
to the face value amount and including the
Embedded derivative assumptions
The estimated fair value of the embedded derivatives related to the issue of convertible loan notes at the point of recognition and at the period end was calculated by using a Black Scholes option pricing model.
Management determined the share price used in the fair value calculation in line with the methods discussed in Note 2 in connection with the ‘Valuation of ordinary shares’, in particular noting the recent valuation obtained from advisers in connection with the planned IPO. As a privately held company, the Group’s share price does not have sufficient historical volatility to adequately assess the fair value of the embedded derivative. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that a volatility of was appropriate for the valuation of embedded derivatives in in existence as at December 31, 2021.
The expected life of the embedded derivative was directly linked to expected redemption dates of the convertible loan note, as noted above.
The Black-Scholes option pricing model requires the use of the risk-free rate of the currency in which the convertible loan note is denominated (US dollars). The Group has applied the appropriate risk-free rate, US treasury bond yields as at the respective redemption dates.
| F-22 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 3. | Revenue |
Year ended December 31, | Year ended December 31, | Year ended December 31 | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Revenue from collaboration agreements | ||||||||||||
The terms of business for payment on satisfaction of a performance obligation are typically 30-60 days.
Collaboration agreements entered into by the Company provide for the entity to work with a partner to carry out collaborative research and development work.
Performance
obligations around upfront payments are deemed to be satisfied over the estimated life of the services promised to be provided. As at
the period end the amount of the transaction price allocated to performance obligations that are unsatisfied totaled £
Performance obligations in respect of contractual milestones are deemed to be satisfied when both parties agree the milestone has been met. Due to the uncertainties around contractual milestones, it is not possible to provide details around the amount of the transaction price allocated to performance obligations that are unsatisfied.
Revenue from reimbursement of research and development costs by collaboration partners is recognized as the costs are incurred.
Details of contract balances at the period end are provided in Note 22. Trade receivables are non-interest bearing. There are no significant financing components included in the contracts.
Amounts outstanding from customers at the year end totaled £(2020: £).
| 4. | Other income |
Year ended December 31, | Year ended December 31, | Year ended December 31, | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Grant income | ||||||||||||
| Other income | - | |||||||||||
Grant income received in the years ended December 31, 2021 and 2020 was represented by payments under the Coronavirus Job Retention Scheme. Grant income received in the year ended December 31, 2019 was represented by research and development related grant funding.
Unrealized exchange differences in the period relate to retranslation of the US dollar denominated convertible loan notes as at the period end.
Other
income includes research and development tax credits totaling £ (2020: £
| F-23 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 5. | Loss before tax |
Loss before tax is stated after charging the following:
Year ended December 31, | Year ended December 31, | Year ended December,31 | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Included in research and development costs: | ||||||||||||
| Depreciation of property, plant and equipment | ||||||||||||
| Amortization of intangible assets | ||||||||||||
| Amortization of right of use assets | ||||||||||||
| Included in administrative expenses: | ||||||||||||
| (Gain)/loss on foreign exchange | ( | ) | ||||||||||
| Depreciation of property, plant and equipment | ||||||||||||
| Amortization of right of use assets | ||||||||||||
| 6. | Finance costs |
Year ended December 31, | Year ended December 31, | Year ended December 31, | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Interest on lease liabilities | ||||||||||||
| Interest on convertible loan | - | |||||||||||
| F-24 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 7. | Income tax credit |
Year ended December 31, | Year ended December 31, | Year ended December 31, | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Current tax | ||||||||||||
| Corporation tax credit | ||||||||||||
| Total current tax credit | ||||||||||||
| Reconciliation of loss before tax to the tax credit for the year | ||||||||||||
| Loss before tax | ||||||||||||
| Loss on ordinary activities multiplied by the standard
rate of tax of | ||||||||||||
| Non-deductible expenses | ( | ) | ( | ) | ( | ) | ||||||
| Deferred tax movement on unrecognized fixed asset differences | ( | ) | ( | ) | ||||||||
| Deferred tax movement on unrecognized timing differences | ||||||||||||
| Deferred tax movement on share-based payments | - | ( | ) | ( | ) | |||||||
| Deferred tax asset not recognized | ( | ) | ( | ) | ( | ) | ||||||
| Additional allowance in respect of enhanced R&D relief | ||||||||||||
| Surrender of tax losses for R&D tax credit refund | ( | ) | ( | ) | ( | ) | ||||||
| R&D tax credits generated | ||||||||||||
| Current tax credit | ||||||||||||
Included
within corporation tax receivable are research and development tax credits of £ (2020: £
Factors affecting future tax
In
March 2021, the U.K. Government announced that from April 1, 2023 the corporation tax rate would increase to
If
the Group’s deferred tax balances at the period end were remeasured at
| F-25 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 8. | Employees |
Year ended December 31, | Year ended December 31, | Year ended December 31, | ||||||||||
2021 Number | 2020 Number | 2019 Number | ||||||||||
| Number of employees | ||||||||||||
| Average monthly number or persons (including directors) employed by the Group: | ||||||||||||
| Research and development | ||||||||||||
| Management, administration and operations | ||||||||||||
Management includes employees who are involved in both research and development and administrative operations.
Year ended December 31, | Year ended December 31, | Year ended December 31, | ||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Staff costs – included in research and development | ||||||||||||
| Wages and salaries | ||||||||||||
| Social security costs | ||||||||||||
| Pension costs – defined contribution | ||||||||||||
| Share based payments | - | |||||||||||
| Staff costs – included in administrative expenses | ||||||||||||
| Wages and salaries | ||||||||||||
| Social security costs | ||||||||||||
| Pension costs – defined contribution | ||||||||||||
| Share based payments | - | |||||||||||
| Staff costs – combined | ||||||||||||
| Wages and salaries | ||||||||||||
| Social security costs | ||||||||||||
| Pension costs – defined contribution | ||||||||||||
| Share based payments | - | |||||||||||
| Total staff costs | ||||||||||||
| F-26 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 8. | Employees (continued) |
Directors’ remuneration | Year ended December 31, | Year ended December 31, | Year ended December 31, | |||||||||
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Directors’ remuneration in respect of qualifying services | ||||||||||||
| Directors’ employer’s pension contributions | ||||||||||||
The
total remuneration of the highest paid or receivable by the highest paid director in the year ended December 31, 2021 was £
| 9. | Basic and diluted loss per share |
Year ended December 31, | Year ended December 31, | |||||||
| 2021 | 2020 | |||||||
| £ | £ | |||||||
| Loss for the year | ( | ) | ( | ) | ||||
| Basic and diluted weighted average number of shares outstanding(1) | ||||||||
| Basic and diluted loss per share | ( | ) | ( | ) | ||||
| (1) |
Basic loss per share is calculated by dividing the loss for the year attributable to the equity holders of the Company by the weighted average number of shares outstanding during the year.
The dilutive effect of potential shares through equity settled transactions were considered to be anti-dilutive as they would have decreased the loss per share and were therefore excluded from the calculation of diluted loss per share.
| F-27 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 10. | Intangible assets |
Software £ | Patent and licence costs £ | Total £ | ||||||||||
| Cost | ||||||||||||
| At January 1, 2020 | ||||||||||||
| Additions | ||||||||||||
| At December 31, 2020 | ||||||||||||
| Additions | ||||||||||||
| At December 31, 2021 | ||||||||||||
| Amortization | ||||||||||||
| At January 1, 2020 | ||||||||||||
| Charge for the year | ||||||||||||
| At December 31, 2020 | ||||||||||||
| Charge for the year | ||||||||||||
| At December 31, 2021 | ||||||||||||
| Net book value | ||||||||||||
| At December 31, 2021 | ||||||||||||
| At December 31, 2020 | ||||||||||||
The amortization charge for the year is recognized within research and development costs in the statements of comprehensive loss.
| F-28 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 11. | Property, plant and equipment |
Facility & Scientific Equipment £ | Computer Equipment £ | Office Equipment £ | Total £ | |||||||||||||
| Cost | ||||||||||||||||
| At January 1, 2020 | ||||||||||||||||
| Additions | ||||||||||||||||
| At December 31, 2020 | ||||||||||||||||
| Additions | ||||||||||||||||
| At December 31, 2021 | ||||||||||||||||
| Depreciation | ||||||||||||||||
| At January 1, 2020 | ||||||||||||||||
| Charge for the year | ||||||||||||||||
| At December 31, 2020 | ||||||||||||||||
| Charge for the year | ||||||||||||||||
| At December 31, 2021 | ||||||||||||||||
| Net book value | ||||||||||||||||
| At December 31, 2021 | ||||||||||||||||
| At December 31, 2020 | ||||||||||||||||
The depreciation charge for the year is recognized within research and development and administrative expenses in the statements of comprehensive loss. Refer to Note 5 for further details.
The
net book value of property, plant and equipment held under sale and leaseback arrangements is £
| F-29 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 12. | Trade and other receivables |
| 2021 | 2020 | |||||||
| £ | £ | |||||||
| Other receivables | - | |||||||
| VAT owed to the Group | ||||||||
| Prepaid clinical trial costs | - | |||||||
| Other prepayments | ||||||||
The fair value of trade and other receivables are not materially different to the book value.
| 13. | Trade and other payables |
| 2021 | 2020 | |||||||
| £ | £ | |||||||
| Trade payables | ||||||||
| Other tax and social security | ||||||||
| Accruals | ||||||||
| Other payables | ||||||||
The fair value of trade and other payables are not materially different to the book value.
| 14. | Convertible loan |
The following table summarizes the changes in the convertible debt instrument during the period ended December 31, 2021
| Host | Embedded derivative | Total | ||||||||||
| loan | £ | £ | ||||||||||
| Balance at December 31, 2020 | ||||||||||||
| Loan notes issued in the period | ||||||||||||
| Accrued interest | ||||||||||||
| Fair value adjustment | ||||||||||||
| Currency adjustment | ||||||||||||
| Balance at December 30, 2021 | ||||||||||||
The
fair value of the residual loan is $
During
2021, the Group issued convertible loan notes with a face value of $
| F-30 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 14. | Convertible loan (continued) |
At the time of an initial public offering (“IPO”),
In the event of an act of default (including if the Group does not list despite its and its bankers’ efforts before February 15, 2022) the outstanding notes become immediately repayable at their face value.
At
the time of our initial public offering on February 10, 2022, loan notes totaling $
The convertible loan has been recognized as a debt instrument with a contingently conversion option separately accounted for as an embedded conversion option derivative.
| (i) | The
convertible loan debt host instrument’s initial fair value is the residual amount of the consideration received, net of attributable
costs of £ | |
| (ii) | The embedded conversion option derivative was initially measured at fair value and is subsequently remeasured to fair value at each reporting date. Under IAS 32 Financial Instruments: Presentation, this derivative could have been classified as a component of equity only if in all cases the contract would be settled by the Group delivering a fixed number of its own equity instruments in exchange for a fixed amount of cash or debt redemption. However, the convertible instrument included a conversion feature resulting in settlement in a variable number of shares and consequently, none of the instrument comprises an equity component. As a result, the derivative is presented in the statement of financial position as a liability in accordance with IFRS 9 and IAS 32. Changes in the fair value (gains or losses) of the derivative at the end of each period are recorded in the consolidated statements of comprehensive loss. |
The value of the embedded derivative is remeasured at fair value at each reporting date (based on a Black-Scholes valuation model) with recognition of the changes in fair value in the consolidated statements of comprehensive loss in accordance with IFRS 9. The inputs associated with calculating the fair value of the embedded derivative are considered to be Level 3 (inputs not based on observable market data) as defined by IFRS 7 – Financial instruments: Disclosures and therefore the valuation of the conversion option is a level 3 valuation. The significant inputs used in the valuation are:
| The model inputs were as follows: | ||||
| 2021 | ||||
| Exercise price in USD | $ | |||
| Share price in USD | ||||
| Time to maturity | ||||
| Expected volatility | % | |||
| Risk free interest rate (US treasury bond) | % | |||
| Dividend yield | ||||
| Probability, as at the reporting date, of IPO completion | % | |||
A change
in the share price input might result in a significantly higher or lower valuation. A % reduction in the share price assumption would
reduce the estimated value of the embedded derivative by £
| 15 | Lease liabilities and similar |
Maturity analysis of leases and similar
| December 31, 2021 | Undiscounted lease payments | Interest | Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
| More than five years | ||||||||||||
| F-31 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 15. | Lease liabilities and similar (continued) |
| December 31, 2020 | Undiscounted lease payments | Interest |
Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
| More than five years | ||||||||||||
The balances relating to lease liabilities and similar can be further analyzed as follows:
Lease liabilities
| December 31, 2021 | Undiscounted lease payments | Interest | Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
| More than five years | ||||||||||||
| December 31, 2020 | Undiscounted lease payments | Interest | Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
| More than five years | ||||||||||||
The principal leasing activities undertaken by the Group relate to the lease of property for the business.
An
incremental borrowing rate of
In
addition, the Group undertakes some sale and leaseback transactions to secure financing. From a review of the sale and leaseback agreements,
it is deemed that as no formal sale has occurred the Group continues to recognize the asset on the balance sheet with a corresponding
liability stated at amortized cost. Liabilities in relation to sale and leaseback transactions totaled £
Sale and leaseback arrangements
In addition, the Group undertakes some sale and leaseback transactions to secure financing. From a review of the sale and leaseback agreements, it is deemed that as no formal sale has occurred the Group continues to recognize the asset on the balance sheet with a corresponding liability stated at amortized cost. There were no gains or losses recognized on sale and leaseback transactions in the period.
| F-32 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 15. | Lease liabilities and similar (continued) |
| December 31, 2021 | Undiscounted lease payments | Interest |
Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
| December 31, 2020 | Undiscounted lease payments | Interest |
Present value | |||||||||
| £ | £ | £ | ||||||||||
| Not later than one year | ||||||||||||
| Between one year and five years | ||||||||||||
Set out below are the carrying amounts of right-of-use assets recognized and the movements during the period:
Buildings £ | Other £ | Total £ | ||||||||||
| At January 1, 2020 | ||||||||||||
| Charge for the year | ( | ) | ( | ) | ( | ) | ||||||
| At December 31, 2020 | ||||||||||||
| At January 1, 2021 | ||||||||||||
| Charge for the year | ( | ) | ( | ) | ( | ) | ||||||
| At December 31, 2021 | ||||||||||||
The following amounts are recognized in the consolidated statements of comprehensive loss:
| Year ended December 31, | Year ended December 31, | |||||||
| 2021 | 2020 | |||||||
| £ | £ | |||||||
| Amortization of right of use assets | ||||||||
| Interest on lease liabilities | ||||||||
Total
cash outflows in respect of leases were £
| F-33 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 16. | Deferred income |
Year ended December 31, 2021
| Contracts with customers | ||||
| £ | ||||
| At January 1, 2021 | ||||
| Released to the statement of profit or loss | ||||
| At December 31, 2021 | ||||
| Current | ||||
| Non-current | ||||
Year ended December 31, 2020
| Contracts with customers | ||||
| £ | ||||
| At January 1, 2020 | ||||
| Released to the statement of profit or loss | ( | ) | ||
| At December 31, 2020 | ||||
| Current | ||||
| Non-current | ||||
Movement in the period reflects the release of deferred income in respect of the long term research and development collaboration agreements. There have been no significant changes in the year.
| 17. | Deferred taxation |
The Group has not recognized a deferred tax asset in respect of tax losses carried forward and other timing differences as at December 31, 2021 on the basis that the availability of future taxable profits against which to offset the losses cannot be determined with reasonable certainty.
The
Group has tax losses carried forward of £
The
unrecognized deferred tax asset at
| F-34 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 18. | Capital and reserves |
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Share capital | ||||||||||||
| 2021 | 2020 | 2019 | ||||||||||
| Number | Number | Number | ||||||||||
| Authorized, allotted, called up and fully paid share capital comprises: | ||||||||||||
| Ordinary shares of £ each | ||||||||||||
| A Ordinary shares of £ each | ||||||||||||
| Total Ordinary share outstanding at the end of the period | ||||||||||||
| Number of | Share capital | |||||||
| shares | £ | |||||||
| Fully paid share capital: | ||||||||
| Balance at December 31, 2019 | ||||||||
| Issue of A Ordinary shares of £ each | ||||||||
| Balance at December 31, 2020 | ||||||||
| Issue of Ordinary shares of £ each | ||||||||
| Issue of A Ordinary shares of £ each | ||||||||
| Balance at December 31, 2021 | ||||||||
Ordinary shares
The Ordinary shares have no specific rights, preferences or restrictions attached to them.
A Ordinary shares
The A Ordinary shares rank equally with all other shares in issue in that on a vote every member has one vote for each share held. During the year to December 31, 2021 the Company issued A ordinary shares at £ each. The A ordinary shares contain preferential economic rights such that, in the event of a share or asset sale (as defined in the Articles of association), they provide a return to the holders of the A Ordinary Shares of an amount greater than or equal to 1.5x the price paid by the investors for A Ordinary Shares. The A Ordinary shares have an anti-dilution provision where shares are subsequently issued at a price below £ per share, whereby the existing A Ordinary shareholders receive additional compensation shares in line with the formula set out in the Articles of Association. The A Ordinary shares rank equally with all other shares in issue with respect to dividends.
Group reorganization
Following a corporate reorganization on December 17, 2021, TC BioPharm (Holdings) plc became the ultimate parent company for the Group. The corporate reorganization has been accounted for as a business combination under common control and therefore, TC BioPharm (Holdings) Limited is a continuation of TC BioPharm Limited and its subsidiaries. The corporate reorganization has been given retrospective effect in these financial statements and such financial statements represent the financial statements of TC BioPharm (Holdings) Limited.
On December 17, 2021 and subsequent to the group reorganization, the Company undertook a share split such that one issued share was exchanged for ten new shares. As a result of the share split, all references in these consolidated financial statements and accompanying notes to units of ordinary shares or per share amounts are reflective of the forward share split for all periods presented.
Nature and purpose of Other reserves
The other reserve arose as a result of the group reorganization described above.
| F-35 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 19. | Share-based payments |
The Group operates an HMRC Approved Enterprise Management Incentive (EMI) share option scheme for employees. Effective 16 December 2014, the Group approved a share option scheme under which the Board of Directors of the Group can award options to directors, officers, employees and consulting personnel of the Group. The Board of Directors will determine the terms, limitations, restrictions and conditions of the options granted under the plan.
The Group has granted options over shares to certain employees. The Group has one stock option plan: the TC BioPharm Limited Enterprise Management Incentive Plan 2014.
The options granted under the EMI share option scheme will typically vest between one and two years after the date of grant. The exception is options granted to senior management that vest immediately. As at the year end, and as at December 31, 2020, all options had fully vested.
| Number of share options | Weighted average £ | |||||||
| Outstanding at January 1, 2021 | ||||||||
| Granted during the period | ||||||||
| Exercised during the period | ||||||||
| Forfeited during the period | ||||||||
| Outstanding at December 31, 2021 | ||||||||
| Exercisable at December 31, 2021 | ||||||||
| Not exercisable at December 31, 2021 | ||||||||
No options were granted or exercised in the period to December 31 2021.
| Number of share options | Weighted average | |||||||
| £ | ||||||||
| Outstanding at January 1, 2020 | ||||||||
| Granted during the period | ||||||||
| Exercised during the period | ||||||||
| Forfeited during the period | ( | ) | ||||||
| Outstanding at December 31, 2020 | ||||||||
| Exercisable at December 31, 2020 | ||||||||
| Not exercisable at December 31, 2020 | ||||||||
| F-36 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 19. | Share-based payments (continued) |
| Number of share options | Weighted average | |||||||
| £ | ||||||||
| Outstanding at January 1, 2019 | ||||||||
| Granted during the period | ||||||||
| Exercised during the period | ||||||||
| Forfeited during the period | ( | ) | ||||||
| Outstanding at December 31, 2019 | ||||||||
| Exercisable at December 31, 2019 | ||||||||
| Not exercisable at December 31, 2019 | ||||||||
The estimated fair value of the options outstanding in the period was calculated by applying a Monte Carlo Simulation for those options issued in 2020 and 2019 and a Black Scholes Model for those options issued in prior periods. The most appropriate approach is selected with reference to the share capital structure at the time of grant. The weighted average fair value of the options at the measurement date during the year ended December 31, 2021 was £ (2020: £and 2019: £) and the weighted average remaining contractual life of . The expense recognized for share-based payments in respect of employee services received during the period to December 31, 2021 is £(2020: £and 2019: £).
The model inputs were as follows: | ||||||||||||
| 2020 | 2019 | |||||||||||
| Weighted average share price | £ | |||||||||||
| Expected volatility | % | % | ||||||||||
| Risk free interest rate | % | % | ||||||||||
| Expected option life | ||||||||||||
| Dividend yield | % | % | % | |||||||||
The weighted average remaining contractual life of the options at December 31, 2021 is years (2020: years and 2019: years).
As at December 31, 2021, as a privately held company, the Company’s share price does not have sufficient historical volatility to adequately assess the fair value of the share option grants. As a result, management considered the historical volatility of other comparable publicly traded companies and, based on this analysis, concluded that a volatility of % was appropriate for the valuation of our share options.
As part of the valuation exercise reference was made to historical share issue prices, taking into account discounts for lack of control and marketability.
Upon vesting, each option entitles the holder to purchase one ordinary share at a specified option price determined at the grant date.
During the year ended December 31, 2020, the Group received services provided by a consultancy business that were settled by providing a right to subscribe for A Ordinary shares at an exercise price of £ per share at a future date, based on certain performance conditions being satisfied. The estimated fair value of the right to subscribe was calculated by applying a Black Scholes Model. This was deemed the most appropriate approach due to the future liquidity event being date-uncertain and could take one of many forms. The share-based payment charge totaled £ (2020: £ and 2019: £).
| F-37 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 19. | Share-based payments (continued) |
The model inputs were as follows:
| 2020 | ||||
| Weighted average share price | ||||
| Expected volatility | % | |||
| Risk free interest rate | % | |||
| Expected option life | ||||
| Dividend yield | % | |||
Group reorganization
Following the year ended December 31, 2021, the Company undertook a group reorganization and a share split such that one issued share was exchanged for ten new shares. The share-based payment disclosures above reflect the .
| 20. | Related party transactions |
The directors and senior executives who have the authority and responsibility for planning, directing and controlling the entity are considered to be key management personnel. Total remuneration in respect of these individuals is disclosed in the table below:
| 2021 | 2020 | 2019 | ||||||||||
| £ | £ | £ | ||||||||||
| Short-term employee benefits | ||||||||||||
| Share-based payments | ||||||||||||
During
the years ended December 31, 2020 and 2021, the Group made purchases of cell culture media from Cell Science & Technology Institute,
Inc., a company in which significant shareholder NIPRO Corporation (Osaka, Japan), has a significant interest in the amount of £
During
the years ended December 31, 2020 and 2021, the Group used consultancy services from Theraldia Consulting Limited a company in which
Dr Alan Clark has a significant interest in the amount of £
During
the year ended December 31, 2020, the executive directors agreed to defer a proportion of their compensation. Repayment of deferred compensation
would be initiated on receipt of an agreed level of funding to support the future capital requirements of the business and settlement
would be staged over twelve months. As at December 31, 2021 the balance outstanding to executive directors totaled £
| 21. | Notes to the cash flow statement |
| 2021 | 2020 | |||||||
| £ | £ | |||||||
| Cash and cash equivalents | ||||||||
Cash and cash equivalents comprise cash and short-term bank deposits with an original maturity of three months or less. The carrying amount of these assets is approximately equal to their fair value.
| F-38 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 22. | Risk management |
The Group is exposed to a variety of risks in the ordinary course of our business, including, but not limited to credit risk, liquidity risk interest rate risk and currency risk, as discussed below. The Group regularly assess each of the material risks to minimize any adverse effects on our business as a result of those factors.
Credit risk
Credit risk is the risk of financial loss to the Group if a customer or counterparty to a financial instrument fails to meet its contractual obligations, and arises principally from the Group’s receivables from customers and from its financing activities, including deposits with banks and financial institutions, foreign exchange transactions and other financial instruments. The Group only engages with banks and financial institutions with a Standard and Poor credit rating of BBB or greater.
The Group has a small number of customers as part of its collaboration agreements. To manage the credit risks around collaboration agreements the Group will assess the creditworthiness of partners as part of the engagement process.
The Group has monitoring procedures in place to identify and follow up on any overdue debts.
Credit risk from balances with banks and financial institutions is managed by the Group’s finance department in accordance with the Group’s policy to only place funds with approved counterparties with the appropriate credit rating.
The Group is exposed to no material credit risk.
Liquidity risk
Liquidity risk is the risk that necessary sources of funding for the Group’s business activities may not be available.
The Group manages liquidity risk by maintaining adequate reserves and reserve borrowing facilities, by continuously monitoring forecast and actual cash flows, and by matching the maturity profiles of financial assets and liabilities.
The Group is utilizing funds raised from issue of equity, collaboration agreements, grant funding and asset finance to support its working capital requirements.
All cash funds are held with a maturity of three months or less.
The following are the remaining contractual maturities of financial liabilities at the reporting date. The amounts are gross and undiscounted, and include estimated interest repayments.
| F-39 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 22. | Risk management (continued) |
Contractual cash flows
December 31, 2021 | Carrying amounts | Total | 2 months or less | 2-12 months | 12-24 months | More 2 years | ||||||||||||||||||
| Financial liabilities | £ | £ | £ | £ | £ | £ | ||||||||||||||||||
| Trade payables | - | - | ||||||||||||||||||||||
| Convertible loan | ||||||||||||||||||||||||
| Other payables | - | |||||||||||||||||||||||
| - | ||||||||||||||||||||||||
December 31, 2020 | Carrying amounts | Total | 2 months or less | 2-12 months | 12-24 months | More than 2 years | ||||||||||||||||||
| Financial liabilities | £ | £ | £ | £ | £ | £ | ||||||||||||||||||
| Trade payables | - | - | - | |||||||||||||||||||||
| Other payables | - | - | ||||||||||||||||||||||
| - | - | |||||||||||||||||||||||
Changes in liabilities arising from financing activities
| January 1, 2021 | Cash flows | New leases | Other | December 31, 2021 | ||||||||||||||||
| £ | £ | £ | £ | £ | ||||||||||||||||
| Current lease liabilities | ( | ) | ||||||||||||||||||
| Convertible loan notes | ||||||||||||||||||||
| Non-current lease liabilities | ( | ) | ||||||||||||||||||
| F-40 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 22. | Risk management (continued) |
| January 1, 2020 | Cash flows | New leases | Other | December 31, 2020 | ||||||||||||||||
| £ | £ | £ | £ | £ | ||||||||||||||||
| Current lease liabilities | ( | ) | ||||||||||||||||||
| Non-current lease liabilities | ( | ) | ||||||||||||||||||
| ( | ) | |||||||||||||||||||
The ‘Other’ column includes the effect of reclassification of non-current portion lease liabilities to current due to the passage of time and the effect of accrued but not yet paid interest on lease liabilities. The Group classifies interest paid as cash flows from operating activities.
Market risk
Market risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market prices. Market risk comprises three types of risk: interest rate risk, currency risk and other price risk, such as equity price risk and commodity risk.
Interest rate risk
Interest rate risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market interest rates. The Group is exposed to no material interest rate risk.
Currency risk
The
Group has transactions denominated in various currencies, with the principal currency exposure being fluctuations in U.S. Dollars and
Euros against pound sterling. The Group’s exposure to the risk of changes in foreign exchange rates relates primarily to the Group’s
Convertible Loan Notes that are denominated in US Dollars and a limited number of supplier agreements denominated in currencies other
than pound sterling. As at December 31, 2021, a 1% increase in GBPUSD exchange rate would reduce the liability for the Convertible Loan
Notes by £
| F-41 |
TC BIOPHARM (HOLDINGS) PLC
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS (CONTINUED)
| 22. | Financial instruments and risk management (continued) |
Equity price risk
The Convertible Loan Notes issued by the Group contain an embedded derivative component that is accounted for at fair value at each period end. A change in the estimated underlying price per share will impact on the valuation of the embedded derivative. As at December 31, 2021, a 5% increase in the estimated share price would increase the value of the embedded derivative by £ and a 5% decrease in the estimated share price would decrease the value of the embedded derivative by £.
| 23. | Capital risk management |
The Group is not subject to any externally imposed capital requirements.
For the purpose of the Group’s capital management, capital includes issued share capital, share premium and all other equity reserves attributable to the equity holders of the parent.
The Group’s objective when managing capital is to safeguard the Group’s ability to continue as a going concern in order to provide returns for shareholders and benefits for other stakeholders and to maintain an optimal capital structure to reduce the cost of capital.
The Group manages its capital structure and makes adjustments in light of changes in economic conditions and the requirement of investors. To maintain or adjust the capital structure, the Group may adjust the dividend paid to shareholders, return capital to shareholders or issue new shares.
| 24. | Subsequent events |
On January 10, 2022, TC BioPharm (Holdings) Holdings Limited was re-registered as a public limited company (“plc”) with the name TC BioPharm (Holdings) plc.
Immediately prior to completion of the Initial Public Offering, TC BioPharm (Holdings) plc re-organized its share capital whereby all of the outstanding series A ordinary shares were re-designated as ordinary shares of TC BioPharm (Holdings) plc on a one for one basis. Immediately prior to the completion of the offering, a further ordinary shares were issued, under the terms of our Articles of Association to certain shareholders who, prior to the IPO, owned A ordinary shares which carried the right, to subscribe at nominal value for a certain number of additional shares, calculated by reference to the pre-money valuation of the IPO.
On February 10, 2022, TC BioPharm (Holdings) plc completed an IPO on Nasdaq, issuing American Depositary Shares (“ADSs”) representing ordinary shares with nominal value of £and warrants to buy ADSs for proceeds before expenses of $million. Funding costs of $million including underwriter fees were incurred.
The ADSs and warrants are considered two freestanding financial instruments because each can be traded separately. The exercise price of the Warrants is $per ADS and will expire on the sixth anniversary of the date of issuance. The exercise price is subject to standard anti-dilutive adjustments in the event of certain stock splits, stock combinations, stock dividends or recapitalizations, and it is also subject to adjustment in certain events specified in the warrant agreement.
Given the warrants include a net settlement clause and the exercise (or strike) price of the warrants is denominated in a foreign currency ($) other than the Company’s functional currency, management concluded that the warrants will be accounted for as derivative financial instruments and presented as a liability on the consolidated statement of financial position with the changes in fair value recognized in the consolidated statement of comprehensive loss.
The relative fair values of the derivative liability and the equity component will be calculated and based on the actual transaction price will be allocated to the equity and the liability components using the relative fair value method.
Following our preliminary valuation, a fair value of $ per each warrant has been identified as at IPO date.
Following the IPO, the value of the embedded derivative was remeasured at fair value by management and deemed to have a value of £, with associated recognition of the changes in fair value being reflected in the consolidated statements of comprehensive loss.
None of the above events are considered to be adjusting post balance sheet events.
| F-42 |